 Home
Home
|
Table of Content - Volume 13 Issue 2 - February 2020
Evaluation of role of partograph in the management of labour in previous caesarean section cases at tertiary care centre
Kiran Mahendra Rajole1, Vaishali Agrawal2*
1Assistant Professor, 2Associate Professor, Department of Obstetrics and Gynaecology, SMBT Institute of Medical Sciences and Research Centre, Dhamangoan, Nashik, Maharashtra, INDIA. Email: drvaishaliagrawal@gmail.com
Abstract Background: Partograph is a composite graphical record of key data (maternal and fetal) during labour, entered against time on a single sheet of paper. Aim: To evaluate the role of partograph in improvement of maternal and perinatal outcomes in trial of labour in women with previous caesarean section (CS). Material and Methods: Hospital based descriptive longitudinal study was carried out at Tertiary Centre. Pregnant women with history of previous CS coming to hospital. Results: Half of women were of age 25 to 29 years. Sixty six percent had FTND, 21.7% had LSCS and 11.6% had forceps assisted vaginal delivery. Mean rate of cervical dilation in vaginal delivery (1.38±0.55) was more than that of LSCS (0.76±0.33) and this difference was statistically significant. Mean rate of descent in vaginal delivery (1±0.48) was more than that of LSCS (0.75±0.39) but this difference was statistically not significant. Among 3 cases with fetal distress, all three were correctly detected by partograph while 66 cases without fetal distress, 11 were wrongly diagnosed as fetal distress by partograph. So sensitivity, specificity, positive predictive value and negative predictive value were 100%, 83.33%, 21.42% and 100% respectively. Conclusion: Utility of partograph can be increased if it is used properly for proper indications at the right time. So partograph is ideal example of appropriate technology in health which can improve perinatal outcome at lowest cost. Key Words: Cervicogram, TOLAC, VBAC, Oxytocin, Scar.
INTRODUCTION In 2014, WHO recommended the use of active phase partograph with a four-hour action line for monitoring the progress of labour.1“Partograph is a composite graphical record of key data (maternal and fetal) during labour, entered against time on a single sheet of paper.”2 Partograph is an inexpensive tool which can effectively monitor labour and prevent obstructed labour when used with standard management protocols. It also increases the quality and frequency of observing mother and fetus in birth canal. Caesarean sections (CS) have become increasingly common in both developed and developing countries.3 Due to epidemic of CS, increasing number of women are facing the issue of mode of delivery in their subsequent pregnancies.4 Maternal complications like Uterine dehiscence and rupture; and perinatal complications like low APGAR score, stillbirths, neonatal deaths and hypoxic encephalopathy are common complications of failed trial of labour. During trial of scar (TOS) or vaginal birth after caesarean section (VBAC), partograph can predict deviation from normal progress of labour early so decision of termination of labour (caesarean section) or augmentation of labour (amniotomy and/or oxytocin) can be made. Present study was undertaken to evaluate the role of partograph in improvement of maternal and perinatal outcomes in trial of labour in women with previous caesarean section.
MATERIAL AND METHODS A hospital based descriptive longitudinal study was carried out for duration of one year at Tertiary Centre in Mumbai. Inclusion criteria were pregnant women with history of previous caesarean section (CS) coming to hospital for delivery and willing for participation. Cases with previous CS where vaginal trial of labour can-not be recommended (e.g. abruption, cord prolapse), Cases with previous CS requiring repeat elective caesarean section (e.g. Placenta previa, malpresentations, Cephalo-pelvic disproportion) and cases with previous CS who did not attain active stage of labour (i.e. 3cm of cervical dilation) (e.g. cases delivered by caesarean before they reached active phase of labour due to protracted latent phase) were excluded. Institutional Ethics Committee (IEC) was taken before the start of study. Written informed consent from each study participant was taken. Thorough clinical examination was conducted to exclude any case with contraindication for trial of labour (TOL). After this, patient was monitored continuously by specialist. Information like demographic characteristics, previous obstetrichistory, type of operation, indication of previous caesarean section, postpartum complications, history of present pregnancy noted on admission. Assessment of vital parameters, uterine activity, scar tenderness, gestational age, presentation, lie, fetal heart rate, cervical dilatation and effacement station were conducted. Information about risk of vaginal trial and possibility of repeat caesarean section was given to patients. Careful monitoring of impending, signs of uterine rupture (i.e. pulserate, fetal heart, scar tenderness, blood pressure, progress of labour) was done. Patients in early labour were examined one hourly and above parameters were noted. Patients attending active stage of labour (i.e. 3cm of cervical dilatation) were attended every half an hourly. The partograph was plotted for these patients starting from zero hour. Referring to ABC of labourcare5, active stage partograph was used. This partograrn was charted from active stage of labour (i.e. 3cm of cervical dilatation). The zero of cervico-gram correspond to the starting of active stage of labour of the patients. It contains only action line, as intervention to accelerate labour in the latent phase is not associated with an improvement in outcome. The two action lines shows, expected progress of cervical dilatation in multiparous (left) and primiparous (right) women. Rates of cervical dilation and descent were recorded. Augmentation with oxytocin and instruments was done where indicated. Maternal morbidities, intra-operative complications, indications for forceps and CS were noted down. Assessment of new-borns were done with APGAR score and other parameters. Microsoft Excel was used for data feeding and analysed with SPSS. V16. Graphs and tables were used at appropriate places to present the data. Descriptive statistics like frequency, proportion, mean and standard deviation were used. Inferential statistics like Chi-square test and student ‘t’ test were used. Statistical significance was set at 5% L.O.S.
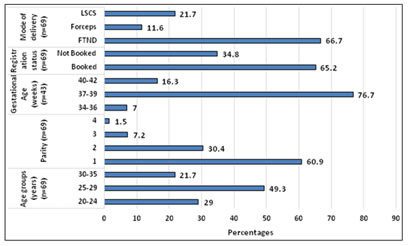
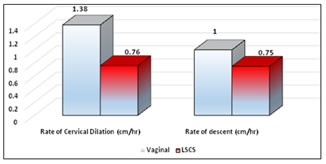
RESULTS Total 69 cases with previous history of LSCS were studied. As shown in figure no.1, 50% women were of age 25 to 29 years followed by 20 to 24 years (29%) and 30 to 35 years (21.7%). Mean age of females was 27.36± 3.89 years. Two third women were booked and rest were not booked. Out of 69 cases, 66.7% had FTND, 21.7% had LSCS and 11.6% had forceps assisted vaginal delivery. Seventy percent cases were pregnant for second time followed by second and third time pregnant females. In 76.7% cases, gestational age was between 37 to 39 weeks followed by 40 to 42 years (16.3%) and 34 to 36 years (7%). Rate of cervical dilation and descent among study subjects shown in table no. 1. Among 19 cases with rate of cervical dilation more than 1.5 cm/hr, rate of vaginal delivery was 100%. Among 28 cases with dilation rate 1 to 1.5 cm/hr, 85.7% had vaginal delivery and 14.3% had LSCS. Rate of vaginal delivery was 100% in cases with rate of descent more than 2 cm/hr. rate of vaginal delivery increased with rate of descent except rate of descent between 1.5 to 2 cm/hr. As shown in figure no.1, mean rate of cervical dilation in vaginal delivery (1.38±0.55) was more than that of LSCS (0.76±0.33) and this difference was statistically significant. Mean rate of descent in vaginal delivery (1±0.48) was more than that of LSCS (0.75±0.39) but this difference was statistically not significant. Out of 15 cases with LSCS, 6 had fetal distress, 5 had meconium stained liquor, 3 had non-progress and 1 had scar dehiscence. Intra-operatively, one case had scar rupture (1.47%), two cases had scar dehiscence (2.87%). In case of scar rupture, partographically scar dehiscence (fetal heart rate deceleration and maternal tachycardia) was detected. In two cases with scar dehiscence, partograph had detected fetal heart rate decelerations. Out of 15 cases with LSCS, 6 had fetal distress, 5 had meconium stained liquor, 3 had non-progress and 1 had scar dehiscence. Among 8 cases with forceps delivery, 1 had fetal distress and 1 had maternal exhaustion and in 6 cases forceps delivery done to cut short 2nd stage of delivery. As indicated in table no. 2, among 3 cases with fetal distress, all three were correctly detected by partograph while 66 cases without fetal distress, 11 were wrongly diagnosed as fetal distress by partograph. So sensitivity, specificity, positive predictive value and negative predictive value were 100%, 83.33%, 21.42% and 100% respectively. One case with tachycardia, correctly detected by partograph while 68 cases without tachycardia, all cases were correctly diagnosed without maternal tachycardia by partograph. So sensitivity, specificity, positive predictive value and negative predictive value were 100%, each (table no.3).
Figure 1: Sociodemographic characteristics of study participants Table 1: Partographic details of study participants
Figure 2: Average duration partographic measurements
Table 2: Detection of fetal distress and maternal tachycardia by partograph
Table 3: Diagnostic value of partograph
DISCUSSION Partograph is important tool for early warning system as it assist in early decision of augmentation and termination of labour serves. It can prevent prolonged labour, can reduce surgical interference also can monitor cases with PROM (premature rupture of membrane).2,6 In present study, rate of VBAC was 78.3%. Sharma et al6 reported 70% incidence of FTND, while forceps delivery in 28% and LSCS in 33.3% cases (before crossing action line). This finding about VBAC (vaginal birth after caesarean section) success in current study were comparable to the studies done by different researchers. 7,8,9,10 Himani et al11 reported mean gestational age of 38.8 weeks. Balachandran et al12 reported vaginal deliveries in 63.6% cases. In current study, half of cases were of age 25 to 29 years with mean age of 27.36 years. Almost three fourth had gestational age of 37 to 39 weeks. Two third were booked and had full term normal delivery (FTND) while 11.6% required forceps delivery and 21.7% required LSCS. Previous study reported, 60-80% success in VBAC.4,7,13 The decision for the elective repeat LSCS or trial of labour in should be based on thorough counselling and careful selection as cases with previous LSCS require special treatment in antenatal care period and during labour.13 In present study with increasing rate of cervical dilatation, chances of vaginal delivery increased proportionately. It was evident that when rate of cervical dilatation was less than 0.5 cm/hr repeat caesarean was required. The association was statistically significant. In study done by Sharma et al6 reported rate of cervical dilatation in forceps it was 1.19±0.23 cm/hour, in full term normal deliveries after previous caesarean section was 1.68±0.24 cm/hour and in repeat caesarean section it was 0.39±0.15 cm/hour. In present study, 48 cases with ARM (artificial rupture of membrane), and 79.2% had vaginal delivery and 20.8% had LSCS. Among 17 cases with ARM and oxytocin injection, 82.4% had vaginal delivery and 17.6% had LSCS. While in 4 cases with no intervention, vaginal delivery and LSCS were done in 50% cases each. Association between intervention and mode of delivery was statistically highly significant. Sharma et al6 reported that incidence of vaginal delivery was increased where labour was augmented by means of oxytocin. They also concluded, oxytocin was found to be a safe and effective means of usual obstetric indications. Himani et al11 reported PROM (83.33%) and prolonged pregnancy (16.66%) as a indications for induction. In current study non-progress was noted in 3 cases. In present study, complications rate was more in babies born to LSCS deliveries. Findings of studies done by Patel et al14, Shah et al13 and Goel et al15 who reported lower complications rates in VBAC compared to LSCS were comparable with present study findings. In current study, only one case was taken for repeat caesarean section for the indication of scar dehiscence. This was detected on partograph by fetal decelerations and maternal tachycardia. Fetal distress was also detected on partograph. When labour progress curve touched the action line of multigravida in partograph, patients were taken for caesarean section for the indication of non-progress. Himani et al11 reported improved neonatal output after using partograph. They reported 3% neonates had respiratory distress and 1% had birth asphyxia while 1 neonate developed transient tachypnoea of new-born. Study done by Khan et al16 reported, The 2 hour and 3 hour lag time after the alert line had a specificity of 78% and 96%, respectively; and a sensitivity of 71% and 43%, respectively, in predicting uterine scar rupture. They concluded that if CS were performed at 2 or 3 h after crossing the alert line, the projected CS rates would have been 36% and 27%, respectively. Partograph had greater sensitivity but lower specificity for detection of fetal distress in present study.
CONCLUSION Present study reported lower rates of prolonged labour and caesarean section among women with previous CS. Partograph proved its utility in current study as LSCS conducted only those who were crossing over alert line on partograph. It also facilitated handover procedure which in turn reflected in lower rates of complications. Partograph had high sensitivity and moderate specificity. Utility of partograph can be increased if it is used properly for proper indications at the right time. So partograph is ideal example of appropriate technology in health which can improve perinatal outcome at lowest cost.
REFERENCES
Policy for Articles with Open Access
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.