 Home
Home
|
Table of Content - Volume 14 Issue 2 - May 2020 Maternal and perinatal outcome in gestational diabetes mellitus in a tertiary care hospital
S N Chaudhari1, Shruti A Gavhane2*
1Professor & HOU, 2Resident Doctor, Department of Obstetrics and Gynecology, Smt.Kashibai Navle Medical College and General Hospital Narhe Pune, Maharashta, INDIA. Email: shruti.lucky5@gmail.com
Abstract Background: Gestational diabetes mellitus (GDM) is defined as a carbohydrate intolerance first diagnosed in pregnancy and may be associated with adverse maternal and perinatal outcome. This study assessed the outcome of GDM. Shortly after delivery, glucose homeostasis is generally restored to normal, but women with GDM are at high risk of developing type 2 diabetes (T2DM). Meanwhile, progressively more data emerge that show that the risk of adverse perinatal outcomes is also associated with degrees of hyperglycaemia. Aim: The aim of the study was to determine the maternal and perinatal outcome in GDM Cases. Materials and Methods: It is a retrospective analysis of women diagnosed with GDM who got antenatal care and delivered in our hospital. GDM was diagnosed based on the 100-gram Oral glucose challenge test i.e. ACOG guideline. Other Medical comorbidities were noted. All the women were followed up till delivery, and the complications were recorded. The baseline characteristics (age, body mass index and parity, mode and time of delivery) were noted in all cases. Total 25 patients met the criteria for GDM out of 200 patients which were screened for GDM. GDM patients were started on diet following which insulin or oral hypoglycaemic agents were given if required. Maternal and perinatal outcome was noted in all women. Results: The prevalence of GDM was 12.5 %. 20 (80%) patients were in age group of 21-25 years.76 % (19) Were having BMI of 18.5 to 24.99. 6 cases had other obstetrics complications. 72 % women received insulin. The glucose values were within the recommended range in 86% of the women. 3 of them had preterm delivery. 32% percent of the women required caesarean section. 7 required admission to the Neonatal Intensive Care Unit. 1 case had IUD and 1 had macrocosmic baby. New-borns of mothers whose GDM optimally treated had less complications. Conclusion: The prevalence of GDM was 12.5% in this study. Adequate treatment of GDM on diet, oral hypoglycaemic agents, or insulin to achieve euglycemia can achieve near-normal maternal and neonatal outcome. The majority of women required insulin for treatment and optimal control of blood glucose resulted in lower neonatal complications. Keywords: Gestational diabetes mellitus, maternal outcome in GDM, neonatal outcome in GDM.
INTRODUCTION Gestational diabetes mellitus (GDM) is defined as carbohydrate intolerance of variable severity with onset or first recognition during pregnancy. Pregnancy is itself a diabetogenic state. The prevalence of GDM varies from 1 to 14%, in direct proportion to the prevalence of Type 2 diabetes in a given population or ethnic group 1. Indian population falls in the high-risk ethnic group for diabetes the recent data on prevalence of GDM in India is 16.55% by WHO criteria of 2hr blood glucose level of 140mg/dl 2. There are controversies about screening, diagnostic tools, and glucose level threshold use as different organizations use different criteria3. GDM is associated with an increased risk of complications for both the mother and the child. The rate of preeclampsia and caesarean section is increased in the mother and the risk of macrosomia is increased in the new born 4. The benefit of blood glucose control during pregnancy has primarily been noted in the reduction of certain neonatal complications such as macrocosmic babies, hyperbilirubinemia, respiratory distress syndrome, shoulder dystocia 5. Our hospital serves underprivileged patients and challenges to treatment exist here. This study was undertaken to study the burden of comorbidities and the outcome of GDM. Most convincing evidence of adverse pregnancy outcome in gestational diabetes was provided by hyperglycaemia and adverse pregnancy outcome (HAPO)6. In India, Seshiah et al... performed a community-based study on the prevalence of GDM in South India and came up with Indian guidelines for GDM which are commonly used in Indian condition .According to this study Medical nutrition therapy is offered to GDM cases first to maintain Fasting BSL <90 mg/dl and post meal glucose <120 mg/dl. If MNT fails to achieve control i.e., FPG ~ 90mg/dl and Post meal glucose ~ 120 mg/dl, insulin may be initiated7.
MATERIALS AND METHODS It was a retrospective cohort study among 200 Antenatal patients screened, 25 GDM patients were diagnosed and were managed and delivered in a tertiary care centre . Another 175 women with normal profile patients without GDM who delivered during the same time. Baseline characteristic of women including age, body mass index (BMI), and parity, mode and time of delivery were taken. Diagnosis of GDM was made by OGTT using 100 g glucose. Patient was labelled as GDM if any two value is more than criteria (fasting blood sugar [BS] ≥95 mg/dl, 1 h BS ≥180 mg/dl, and 2 h BS ≥155 mg/dl and 3 h BS ≥ 140). Initially, patients were started on diabetic diet with some physical exercises. Diet was started by a dietician. If BS levels were not controlled on diabetic diet, then women were either started on oral hypoglycaemic agent or insulin. GDM was considered to be optimally controlled if the fasting glucose (FBS) was <95 mg/dl and 2nd h postprandial glucose (PPBS) was <120 mg/dl as defined 8. All the women were followed up till delivery and the maternal and fetal outcomes were recorded. The women received regular antenatal care. Any antenatal complications were noted and treated, particularly urinary tract infection (UTI), candidiasis, preeclampsia, hypothyroidism etc. Shoulder dystocia was defined as a vaginal cephalic delivery that requires additional obstetric manoeuvres to deliver the fetus after the head has delivered, and gentle traction has failed (8). Macrosomia was defined as birth weight >4 kg. Neonatal hypoglycaemia was defined as plasma glucose level <45 mg/dl by point of care glucose testing later confirmed by laboratory testing 9. As a protocol, all patients with GDM on insulin were induced at 38 weeks, and those controlled on diet were induced at 39-week period of gestation if not in labour before this period. The study was approved by the Institute ethics committee, and a written informed consent was obtained from the women. Maternal complications during pregnancy and during delivery were recorded. The neonatal complications were recorded. INCLUSION CRITERIA: All patients attending the antenatal OPD of tertiary health care centre. EXCLUSION CRITERIA: All pregnant patients with
OBSERVATIONS AND RESULTS Out of a total of 200 women who were screened For GDM, 25 women developed GDM as per criteria using 100 g OGTT making prevalence to be 12.5% A total of 4 (16%) were controlled on diet, whereas 18 (72%) required insulin and 3 (12%) were treated with oral hypoglycaemic agent (metformin).
Table 1: Treatment Given for GDM cases.
Table 2: Age distribution of cases studied in the study group.
Of 200 cases studied, 15 (7.5%) had age between 18 – 20 years, 161 (80.5%) had age between 21 – 25 years, 19 (9.5%) had age between 26 – 29 years and 5 (2.5%) had age above 30 years. The mean ± SD of age of cases studied in the entire study group was 25.1 ± 3.4 years and the minimum – maximum age range was 18 – 37 years. Maximum no. cases of GDM 20 i.e. 80 % where in age group of 21-25.
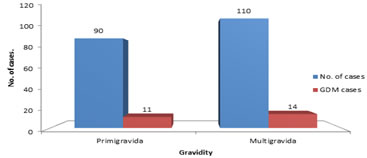
Gravidity distribution of cases studied in the study group. Of 200 cases studied, 90 (45.0%) were primigravida and 110 (55.0%) had multigravida in the study group.14 i.e 56% GDM cases where multigravida and 11(44%) were primigravida. Figure 1: Gravidity distribution of cases studied in the study group.
Table 3: Distribution of body mass index (BMI) among the cases studied in the study group
Of 200 cases studied, 5 (2.5%) had BMI less than 18.50 kg/m2, 158 (79.0%) had BMI between 18.50 – 24.99 kg/m2, 31 (15.5%) had BMI between 25.00 – 29.99 kg/m2 and 6 (3.0%) had BMI above 30.00 kg/m2 in the study group. 76%-19 cases of GDM where having BMI of 18.5 to 24.99 kg/m2 Table 4: Distribution of cases as per mode of delivery
Among 200 study subjects, 114 cases(57%) delivered vaginally , 37 % cases caesarean section and Instrumental deliveries were 12(6%) .14 cases i.e 56% of GDM underwent vaginal delivery, 3 (12%) cases underwent Instrumental delivery and 8 i.e 32% underwent LSCS. Table 5: Distribution of cases as per of time of delivery
The majority 189 (94.5%) were term deliveries and 11 (5.5%) were preterm.3 (12%) of GDM cases were preterm and 22 (88%) were term.
Table 6: Distribution of obstetric complications among the cases studied in the study group
Of 200 cases studied, 171 (85.5%) did not have any complication, 13 (6.5%) had severe anaemia, 5 (2.5%) had gestational hypertension, 4 (2.0%) had pre-eclampsia, 1 (0.5%) had epilepsy and 6 (3.0%) had other complications in the study group. Out of which 19 (76%) ,2 (8%) cases had gestational hypertension ,3(12%) cases had pre-eclampsia and 1 (4%) had hypothyroidism. Perinatal outcome and neonatal complications in two group
Table 6: Association of APGAR score
In 25 cases of GDM 19 had APGAR <7 at 1 min and 2 GDM cases had APGAR <7 at 5 min.
Table 7: Neonatal Complications in two groups
In this study 1 had macrosomia,7 neonates required NICU admission in which 3 had respiratory distress ,2 had hypoglycaemia, 2 had IUGR.1 GDM case had IUD as she also had severe preeclampsia and lost to follow up after 33 weeks.
DISCUSSIONThe main aim was to compare maternal and fetal outcomes in cases diagnosed as Gestational diabetes mellitus either by “Oral Glucose Tolerance Test’’(OGTT). Gestational diabetes mellitus (GDM) is common problem in pregnancy. However, controversies exist regarding adverse effects of GDM due to the use of different criteria used by different studies and various confounding factors in these studies. The incidence of GDM in the present study was found to be 12.5% which was similar to that of 13% by Nair et al. 10 Pregnancy induced hypertension In the study, be Saxena et al., the incidence of PIH was 40% 11. According to Wahi et al. in Jammu, India it was 6.45% (12). Xiong et al. reported mothers with GDM were at increased risk of presenting with pre-eclampsia as they have similar risk profile 13. In the present study, 20 % (8% had gestational hypertension and 12 % preeclampsia) patients had pregnancy complicated by both GDM and PIH. But majority patients had no PIH in present pregnancy. No statistically significant difference was seen between both groups(p=0.61). Thus, there is an association between PIH and GDM and early diagnosis and initiation of treatment should be done to improve the outcome. Preterm delivery In a study by Mahalakshmi et al., 19% were preterm live birth.14 Saxena et al. reported a 12% incidence of preterm babies 11 In the present study, Preterm delivery was seen in 12%. Preterm births in present study were attributed to premature preterm rupture of membranes, preterm labour and early induction in cases of severe preeclampsia. No pregnancy was continued till post datism as chances of IUFD are increased. Mode of termination According to Kale et al., the incidence of LSCS in patients with GDM was found to be 60% 15. According to Saxena et al.., caesarean was done in 42% cases (11). Wahi et al. reported 22.58% incidence of caesarean (12). Cassey et al. reported caesarean section rates of 30% in women with GDM.16 A study in Denmark by Jenson et al., and in Sweden by Aberg et al. also found an increased rate of caesarean section in patients with GDM. 17,18 In the present study, 32 % patients of underwent LSCS. 68 % delivered vaginally. Difference was not statistically significant (p=0.21). Macrosomia In study by Cypryk et al., history of big baby (macrosomia) was present in 11% of patients (19). Najafian et al. found incidence of macrosomia in 9% cases (20). Balaji et al. found incidence of macrosomia in India as 9.9% (21). In present study, macrosomia was seen in 4% of baby. Difference was not statistically significant. Gestational diabetes, maternal obesity (BMI), maternal age and positive history of previous macrosomia were the major risk factors for macrosomia which were compared with the normal weight infant groups. Fetal macrosomia is a common adverse infant outcome of GDM if unrecognized and untreated in time. For the infant, macrosomia increases the risk of shoulder dystocia, postpartum haemorrhage and genital injury. Neonatal complication Mitanchez in literature review found there was limited data from which to report on the prevalence of respiratory distress in infants born to mothers with GDM.22 In present study 3 cases had respiratory distress syndrome. Malak et al. noted the incidence of neonatal intensive care admission was 4.9%.23 In our study 28% had NICU admission. Mitanchez et al.22 observed that untreated moderate or severe GDM increased the risk of fetal and neonatal complications. However, the risk of neonatal complication and macrosomia was minimal with adequate treatment. They found a relationship between maternal blood glucose levels and increased birth weight. Treatment of GDM reduces the risk of macrosomia and adverse neonatal outcome.
CONCLUSIONGDM is a window of opportunity for prevention of diabetes in future life but this opportunity provided by GDM can be utilized only if optimal medical and obstetric care is provided to the antenatal patient with GDM. Optimal management of GDM remains a challenge for the obstetricians and endocrinologists. There is a higher prevalence of GDM in India which varies from area to area and socioeconomic status. Adequate treatment of GDM on diet, oral hypoglycaemic agents, or insulin to achieve euglycemia can achieve near-normal maternal and neonatal outcome. Although birth weight and neonatal hypoglycaemia remain higher in GDM patients.
LimitationsA limit of our study is the retrospective nature of the analysis and the lack of data on maternal weight gain during pregnancy and lack of data on the ponderal index of the newborn. Lack of in-house endocrinologist for consultation at our institute. REFERENCES
Policy for Articles with Open Access:
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.