 Home
Home
|
Table of Content - Volume 14 Issue 2 - May 2020
A study on anomalies in newborns and their association with feto-maternal factors
Shaifali Singhal1, Nirav Garala2*, Kamal Goswami3, Kavita Dudhrejia4
1IIIrd year resident, 2Assistant Professor, 3Professor and HOD, 4Associate Professor, Department of Obstetrics and Gynaecology, P.D.U. Medical College & Civil Hospital, Rajkot, Gujarat, INDIA. Email: shaifali911@gmail.com
Abstract Background: Prospective observational study carried out among total 12,240 registered deliveries in Department of obstetrics and gynaecology in civil hospital, PDU medical college, Rajkot in Gujarat with the objectives of incidence of congenitally malformations, Assessment of high risk feto-maternal factors in patients with congenital malformation and association between maturity and congenital malformation. Majority of women who delivered malformed babies that was 36 (45 %) were between 26-30 years age group, minimum number of women with malformed baby that was 3 (3.7 %) belongs to age group >35 years. About 73.75 % of congenital malformation were found in multipara while 26.25 % were in primipara. In total malformed babies delivered maximum were of 1.5-2.5 kg weight i.e. 39 (48.75 %), minimum were of <1 kg i.e. 2 (2.5 %), and in 1-1.5 kg group 5 (6.25 %), in 2.5-3 kg were 20 (25 %), of more than 3 kg were 14 (17.5 %). ‘fetal screening programs’ and ‘birth defects preventive programs’ can be catered to particular population, based on the prevalence of the type of defect and availability of the local sources. Keywords: preterm maturity, Low Birth weight, congenital anomaly
INTRODUCTION Congenital malformation in newborns are one of the major public health problem in India as well as around the world. They have a leading role in perinatal and infant morbidity and mortality. Many survivors are physically and/or mentally handicapped. This has a great social, psychological and economical impact on family. In India congenital anomalies contribute 8-15% of perinatal deaths and 13-16% of neonatal deaths in India.1,2As congenital anomalies are one of the main causes of infant death and poor health for the children with congenital anomalies, epidemiological research of congenital anomalies is significant for the field of reproductive and perinatal health.3,4 Aim and Objectives
METHODOLOGY This was a prospective observational study carried out among total 12,240 registered deliveries in Department of obstetrics and gynaecology in civil hospital, PDU medical college, Rajkot in Gujarat during the period of October 2017 – March 2019 over a period of one and a half year.
OBSERVATION Total 12,240 registered deliveries in Department of obstetrics and gynecology in civil hospital, PDU medical college, Rajkot in Gujarat during the period of October 2017 – March 2019 over a period of one and a half year. Table 1: Incidence of congenital anomalies
Total 12,240 births were recorded in which 80 births those were detected with congenital anomalies had gestational age more than 28 weeks.
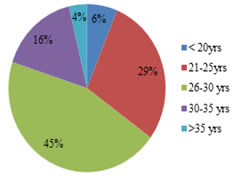
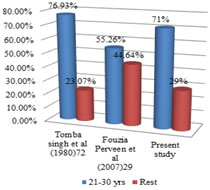
Graph 1: Age wise distribution of women with Graph 2: Comparison of studies of age wise distribution congenital fetal anomalies of women with congenital fetal anomalies
Graph 2 shows, women with malformed babies belongs to age group 21-30 yrs was 73.75 % which also favours the results of studies of Fouzia Parveenetal (2007)5of 55.26% and Tomba Singhetal (1980)6of 76.93%. In this study out of all age groups, number of malformed babies was maximum in age group 26-30 years which was 36 (45%) and minimum in age group of >35 years which was 3 (3.7%). Out of all age groups, incidence of malformed babies was maximum in age group >35 years which was 3.9 % and minimum in age group of <20 years which was 0.4 %. This indicates pregnancy in women having age more than 30 yrs had more chances of having anomalous baby.
Table 2: Parity wise distribution of women with fetal anomalies
In this study, out of total malformed babies maximum babies were born to third or more para which was 40 (50%) and minimum were second para 19 (23.75%) and primipara were 21(26.25%).
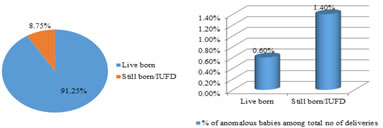
Graph 3 indicates that about 91% of delivered babies were live born, while rest of them about nearly 9% of them were still born or belongs to IUFD. Out of this 8.75 % of anomalies, 0.6% were live born and 1.40% were stillborn or IUFD.
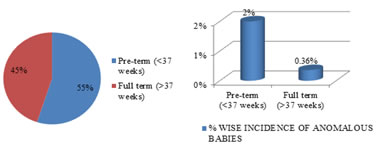
Graph 4: Maturity and congenital malformation This graph shows the importance of maturity of the fetus directly correlates the healthy status of fetus. About 55% of delivered babies were preterm while rest of them were full term that was about 45%.
Table 3: Comparision of maturity and congenital malformation
In this study chi square value = 76.51, p value = Zero, so the association is significant. A p-value less than 0.05 (typically ≤0.05) is statistically significant. So it can be concluded proportion of babies reaching term in anomalous babies was significantly lower than term babies in normal babies. In this study positive association was found between congenital malformation and prematurity. This was particularly a cause of concern as prematurity and stillbirths were a major cause of perinatal mortality. Similar findings were also obtained in other studies such as Doddasbasappa et al. (2017)7.
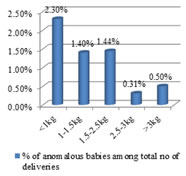
Graph 5: Comparison of birth weight and congenital malformation
In this study incidence of malformed babies was more in <1kg babies and minimum in 2.5-3kg, this was comparable to the study done by Taskande et al. (2010)8. In this study chi square value = 1.68, p value = 0.194, association was significant. So it can be concluded that proportion of low birth weight babies (<2.5kg) in anomalous babies was significantly higher than in normal babies. In this study positive association was found between congenital malformation and low birth weight. Low birth weight was associated with increased risk of congenital malformations. Fetal malformations (chromosomal and non chromosomal) account from 15-20% of IUGR cases with low birth weight. This highlights the fact that the presence of congenital anomaly it self hampers the growth of a developing foetus. This fact was also highlighted in other studies such as Taksande A et al. (2010).8
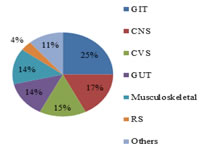
Graph 6: System-wise incidence of congenital anomalies
In this study out of all malformation 20 (25%) were involving GIT system, 14 (17.5%) were involving CNS and neural tube defects, 12 (15%) involving CVS, 11 (13.75%) involving musculoskeletal system, 3 (3.7%) involving respiratory system and 9 (11.25%) involving other systems.
SUMMARY In total 12,240 births were recorded in which 80 births were those detected with congenital anomalies had gestational age more than 28 weeks. This gives a birth Incidence in percentage of congenital anomalies from total birth in institute was 0.653%. Majority of women who delivered malformed babies that was 36 (45 %) were between 26-30 years age group, minimum number of women with malformed baby that was 3 (3.7 %) belongs to age group >35 years. About 73.75 % of congenital malformation were found in multipara while 26.25 % were in primipara. 76 % of total malformed babies belong to Hindu community more than Muslim 13 %. In total malformed babies 73 (91.25 %) were live born and 07 (8.75 %) were still born. 8. In total malformed babies 55 % i.e. 44 were preterm, and 45 % i.e 36 were fullterm. In total malformed babies delivered maximum were of 1.5-2.5 kg weight i.e. 39 (48.75 %), minimum were of <1 kg i.e. 2 (2.5 %), and in 1-1.5 kg group 5 (6.25 %), in 2.5-3 kg were 20 (25 %), of more than 3 kg were 14 (17.5 %).. In this study total 20 (25 %) malformation were involving GIT, 14 (17.5 %) were involving CNS and neural tube defects, 12 (15 %) involving cardio vascular system, 11 involving musculoskeletal system, 3 involving respiratory system and 9 involving other systems.
CONCLUSION Screening should detect risk factors not only antenatally but also prenatally, ‘fetal screening programs’ and ‘birth defects preventive programs’ can be catered ton particular population, based on the prevalence of the type of defect and availability of the local sources. Public health promotion and education programs on sexual and reproductive health, attention should be directed not only to factors related to contraception, family planning, infertility, but also issues on avoidable risk factors for congenital anomalies and prevention options should be emphasized.
REFERENCES
Policy for Articles with Open Access:
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.