 Home
Home
|
Table of Content - Volume 14 Issue 3 - June 2020
A validation study of confidential enquiry into maternal and child health recommended modified early obstetric warning system in a tertiary care hospital
Abirami Gobinathan1*, Poornima M2
1Final Year Postgraduate, 2Associate Professor, Department of Obstetrics & Gynaecology, Jagadguru Sri Shivarathreeshwara Medical College, Mysore-570004, INDIA. Email: abiramigobinathan@gmail.com
Abstract Background: Modified Early Obstetric Warning System (MEOWS) chart adopted from the year 2003 to 2005 “Confidential Enquiry into Maternal & Child Health report” is based on the fact that critical illness follows physiological parameters abnormality. The “Trigger” in this chart helps in the early recognition of maternal morbidity thereby halting the progress to severe maternal morbidity and mortality. Objective: To validate MEOWS chart as a bedside screening tool for predicting early obstetric complications, which helps in timely intervention and treatment. Materials and Methods: It was a explorative study conducted in inpatients of a tertiary care hospital from January 2018 to June 2019. Physiological parameters of 400 women (including pregnant women from twenty weeks gestation to six weeks postpartum) were recorded on MEOWS chart. A trigger was defined as “one markedly abnormal parameter (red trigger) or the combination of two simultaneously mildly abnormal parameter (two yellow triggers)”. Chi Square test and test for proportion were used. Results: 101 (25.3%) women were triggered to abnormal zones on this chart. 96 (24%) women had fulfilled obstetric morbidity definition. MEOWS chart carries high sensitivity of 95.83% and high specificity of 97.04% with a high positive and negative predictive values of 91% and 98.6% respectively for predicting obstetric morbidity. Individual parameter of MEOWS chart significantly correlated with obstetric morbidity. Conclusion: Hence MEOWS chart is validated as a bedside screening tool useful for predicting obstetric morbidity. It can be routinely used in every obstetric unit to reduce maternal mortality. Key Words: MEOWS, Obstetric morbidity, CEMACH, Trigger
INTRODUCTION Child bearing is a normal physiological event, which should ensure woman, a healthy pregnancy, childbirth and postnatal recovery. Death due to pregnancy and childbirth may happen due to complications that are preventable or treatable. Recording physiological parameters is an integral part of antenatal care. As pathological abnormalities precedes clinical illness, it helps in early identification of women at risk so that they can be transferred to a higher centre on time.1 Several variants of early warning charts are available in the developed countries, for decades, for use in adult non-pregnant patients. They are used for evaluation of physiological parameters to identify patients who can become severely ill and may require additional interventions or escalated care. However these charts cannot be used in pregnant women because the normal physiological changes in pregnancy are not taken into consideration in the construction of these charts2. The “Confidential Enquiry into Maternal and Child Health”, April 2003, The United Kingdom review of maternal deaths “Saving Mothers’ Lives” and “The Maternal Critical Care Working Group” recommended the MEOWS to be introduced in all obstetric inpatients to help early identification and treatment of deteriorating parturient.3 MEOWS is an easy way to record the physiological parameters and to identify the pregnant women who require urgent intervention.4,5 MEOWS also helps in optimal utilization of available health resources particularly in developing countries like India where health resources are scarce.
AIM OF STUDY The aim our study is to validate MEOWS chart as a bedside screening tool for predicting early obstetric complications, which helps in timely intervention and treatment.
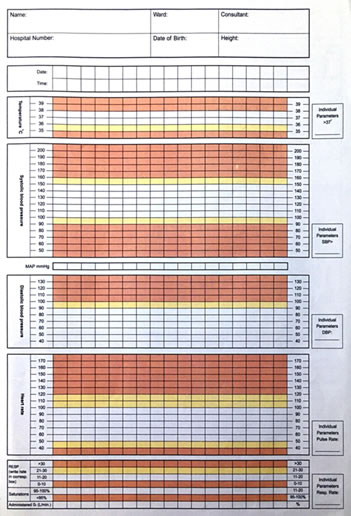
MATERIALS AND METHODS This was a prospective observational study undertaken in the Department of Obstetrics in a tertiary health care referral centre from January 2018 to June 2019. Study population: 400 (Krejice and Morgan table 1970) Inclusion criteria: All inpatient women between 20 weeks gestation to 6 weeks post partum. Exclusion criteria: Chronic systemic illness patients – cardiac, respiratory, neurological, etc, Subjects were explained about the study and written informed consent were taken. A thorough clinical evaluation was done following admission comprising of the following details: Age, socio economic status, booked/ unbooked, obstetric code, period of gestation. Detailed history including past obstetric events, menstrual history, past history, family and personal history. Detailed physical examination was performed including Systolic Blood Pressure, Diastolic Blood Pressure, Heart Rate, Respiratory Rate,SPO2and Temperature, obstetric examination was done and the observations were entered in the MEOWS chart(Fig. 1, 2).
Figure 1: MEOWS CHART page 1
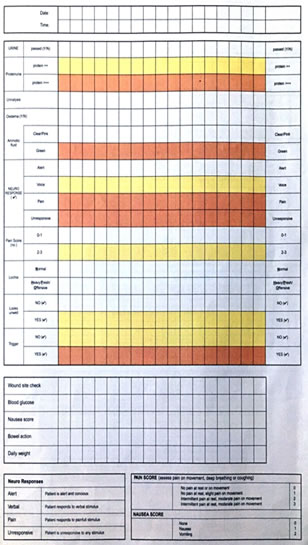
Figure 2: MEOWS Chart Page
First entry was made at the time of admission. The frequency of entry in MEOWS chart depends mainly on the severity of the condition with which the patient got admitted or atleast every 12th hour. During labour, partogram was used. In the recovery room again entries were made in the MEOWS chart before shifting the patient to postnatal ward. In the post natal ward also, daily observations were recorded 12th hourly till the patient was discharged. A trigger was defined as “a single markedly abnormal observation (red trigger) or the combination of two simultaneously mildly abnormal observation (two yellow triggers)”. Based on observations patients are categorized as triggered and non triggered. Outcome is measusered based on Obstetric morbidity among the triggered patients. The physiological parameters were correlated with the obstetric morbidity. Obstetric morbidity were diagnosed by definitions as in Table no. 1
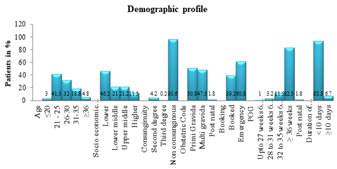
RESULTS Completed MEOWS chart of 400 study subjects were analyzed using SPSS version 16.0. For data description, “descriptive statistics, frequency analysis, percentage analysis were used for categorical variables and the mean and S.D were used for continuous variables”. The significance in categorical data is found by Chi-Square test and test for proportion were used. Study population was largely comprised of antenatal (98.25%), Young females between 21 to 25 years of age (41.5%), belonging to lower socioeconomic status (46.2%). About 60.8% of the women had regular antenatal visits at the same centre and most of them were primigravidas (50.8%). Associated obstetric condition was present in 26.5% of the cases with hypertensive disorders (21.5%) being most common . Associated medical conditions were present in 16.2% of cases with hypothyroidism (10%) being the commonest follow. (Figure 3). Figure 3: Demographic Profile
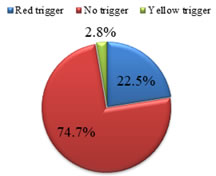
Of all the Meows chart entered there were a total of 25.3% (101 women) were triggered. Of the triggered patients red triggered patients were 22.5% (90 women) and yellow triggered patients were 2.8% (11 women). (Figure 4) Figure 4: Trigger
The major triggered physiological parameters as seen in table no. 2 were systolic blood pressure (21.05%), diastolic blood pressure( 20.25%), proteinuria(18%) , heart rate(12.8%), and amniotic fluid (10.3%). 25.3% of women were triggered to abnormal zones at or after admission. 24 % (96 women) fitted out the criteria for obstetric morbidity. Obstetric interventions among the triggered patients were emergency LSCS (79.21%), ICU admissions (7.92%), blood and blood products transfusion (34.65%), MgSO4 administration (26.73%) and ventilator support (1.98%). 80% were term neonates and 20% were preterm. 59% were healthy neonates and on mother’s side and 35.5% had NICU admission and 5.5% were dead. Meows chart was found to be 95.83% sensitive and 97.04 % specific and had positive predictive value of 91.09 % and negative predictive value of 98.66 %
DISCUSSION The use of Early warning systems for patients can be traced back to a paper in 1999.[2] The idea behind EWS arose from the knowledge that physiological abnormalities precede critical illness. Early warning systems to detect critical illness in obstetric patients have been specifically designed because:
The 2003–2005 triennial Confidential Enquiry into Maternal and Child Health (CEMACH) report recommended the routine use of the modified early obstetric warning system (MEOWS), which is an early warning system adapted for the obstetric population.8,9 The parameters in MEOWS are designed to detect patients suffering from conditions that may lead to severe maternal morbidity and mortality. The parameters in MEOWS seek to identify patients with hypertensive disorders, hemorrhage, thromboembolism, sepsis, and cardiovascular and cerebrovascular complications, conditions that account for more than 50% of all maternal deaths and disproportionate major morbidity.1,10 The present study was carried out on 400 obstetric admissions mainly comprising women of 20 to 30 years(73.5%) , maximum antenatal women (98.25%) of lower socio economic class (46.2%) with 60.8% were booked with maximum in their third trimester (97.2%). The demographic profile of present study was similar to a study conducted in Delhi by Anju Singh et al..11 A similar validation study conducted in Coimbatore included 189 study subjects with majority between 20 to 30 years (67.1%) with mean age of 26 years belonged to lower socio economic status (49.7%) with maximum booked cases (68.25%) in their third trimester (91.5%)12 The most frequently triggered physiological parameter in our study was high blood pressure ( 41.3%) followed by abnormal heart rate (12.8%) which coincides well with study by singh et al. – high BP (42%) and abnormal heart rate(28%) and Anju singh et al. – high BP (37.3%) and heart rate (19.4%)4,11 The most commom morbidity in our study was hypertension (75%) followed by haemorrhage (20.2%) , puerperal sepsis (1.92%) and others (2.8%) which is similar to a study in Delhi – hypertension (69.4%) , haemorrhage ( 9.6%) , puerperal sepsis (2.26%) and others (18.08%) whereas in a study by singh et al. haemorrhage was the most common cause of morbidity (43%) followed by hypertension (31%) , infection (20%).4,11 The obstetric interventions in our study included emergency LSCS (79.21%), ICU admissions (7.92%), blood and blood products transfusion (34.65%), MgSO4 administration (26.73%) and ventilator support (1.98%) whereas in Anju singh et al. study the interventions were emergency LSCS in 28.9% and blood and b;lood products transfusion in 20.4%.11 The sensitivity and specificity in our study was 95.8% and 97.04% respectively which is comparable with studies by Singh et al.. and Anju Singh et al..4,11
CONCLUSION MEOWS, being an objective way of assessing the health status, is a very reliable tool for assessment both in Community as well as in hospital set up. It picks up alteration in physiological parameters before signs and symptoms develop thereby helps in early referral of patients to higher centre for expertise care. MEOWS helps in early identification of disease that leads to morbidity and mortality during pregnancy and may help in planning National Programmes aimed at preventing those diseases and to devise Nationwide Guidelines for the treatment of those illness during pregnancy. Reduction of maternal morbidity indirectly reduces neonatal morbidity and mortality –leading to a safe motherhood and a healthy environment to the newborn.
ACKNOWDLEDGEMENT: I thank my Guide and my family for their constant support.
REFERENCES
Policy for Articles with Open Access:
|
|

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.