 Home
Home
|
Table of Content - Volume 16 Issue 2 - November 2020
Perspective study on vaginal, vulvar disorders in Kerala population
Vijayadevi1*, Jayasabarinathan M2
{1Assistant Professor, Department of Obstetrics and Gynecology} {2Professor, Department of Anatomy} Mount Zion Medical College, Adoor, Kerala, INDIA. Email: viji.mmc03@gmail.com
Abstract Background: Due to unhygienic, illteracythere are many infections, on-infections, fungal, Infections which are usually ignored by females. Due to their busy schedule of their domestic commitments Method: 125female aged between 16-66were studied and classified into three group (a)16-24 (b) 25-45 (c)46to66 age group vaginal pH was measured by pH indicator strip bimanual examination. Swab was collected from posterior vaginal fornix sent for Amine test and gram staining and culture to rule out bacterial vaginitis. For fungal sawb was incubated on SDA. Incubated 37oc and observed till 4 weeks. Vulvular biopsy was done in vulvular dystrophy or if malignancy was suspected Results: In 16-24 age group 11(34.3%) had bacterial infection, 9(28.1%) had fungal infection 7 (21.8%) had allergic conditions 3(9.37%) had herpes, 2 (6.25%)had malignancy in age group 25-45, 15(35.7%) had bacterial infection 13 (30.9%) had fungal infection 6(14.2%) had allergic condition 5(11.9%)herpes , 3(7.1%)had malignancy. In the age group 46-66 20(39.2%) had bacterial infections, 14(27.4%)had fungal infections 6(11.7%)had allergic condition, 4(7.84%) had herpes 7(13.7%) had malignancy. Conclusion: prevalence and risk factors associated with infections causes vagino-vulvular among reproductive and post menopausal are still unclear. Therefore present study will highlight vagino-vulvular disorders at different age group. Key Words: bacterial infections, vulvo vaginal conditions, allergic conditions, herpes, malignancy.
INTRODUCTION Infection or inflammation of vagina or vaginitis caused by various infections or non- infections factors1 The most of the common causes are bacterial vaginosis (BV), valvo-vaginal candidiasis (VVC) and Trichoma vaginitis (TV)2 BV is most commonly asymptomatic characterized by discharge of homogenous grayish-whitesmelly secretion fishysmell after intercourse or during menstruation and elevation of PH above 4.53)VVC caused by over growth of yeast, mainly candida albicans4 TV is flagellate protozoan parasite that causes trichomanasis, characterized by sever vaginitis. Its transmission is usually sexual and frequent recurrence if the male partner is not simultaneously treated women with Tv may complain foul smelling discharge, dysuria, dyspareunia, vulvar itching and pain. The vuvula may be erythematous, edematous and excoriated and sub epithelial hemorrhages or strawberry spots may be absorbed on the vagina and cervix5 If these disorders are not treated may cause morbidity and mortality in later days.
MATERIAL AND METHOD 125 females visiting to Obstetrics and Gynecology department of Mount Zion Medical College, adoor, Kerala, were studied. Inclusive Criteria – women having vulvar and vaginal irritation, itching burning pain and/or dyspareunia (painful intercourse) were included in the study exclusion criteria- patients having pregnancy HIV positive were excluded from the study Method – detail history of each patient was noted, The quantity odour , colour and consistency vaginal discharge was noted. The vaginal pH was measured directly using pH indicator strip against posterior fornix. A bimanual examination was done to look for any Adnexal tenderness. Clinical investigations were vaginal swabs from the posterior vaginal fornix were collected before bimanual examination. One swab was sent for amine test and preparation of wet mounts. The second ( another swab) was sent for Gram staining and culture to rule out bacterial vaginaosis from amine test .The wet mount test to identify the presence of motile, Trichomonos and clue cells. Gram staining to confirm the presence of clue cells budding yeast cells and pseudohyphae To rule out the secondary bacterial infection. The swab was inoculated on blood agar and Macon key agar, incubated at 37oc for 18 hours and plates were studied and confirmed by a battery of biochemical reactions for fungus, swab was inoculated on SDA, incubated at 37ocand observed till 4 weeks and growth was confirmed by germ tube test, Valvular biopsy is done in cases where vulvular dystrophy or malignancy is suspected. The study was May 2019 to April 2020. Statistical analysis – The different age group and different diseases were classified with percentage. The statistical analysis was in SPSS software. This research paper is approved by Ethical Committee of Mount Zion Medical College, Adoor, Kerala-691556
OBSERVATION AND RESULTS TABLE 1: Study of Vagino – Vulvular disorder in the age group 16-24. (Total no of patients 32)
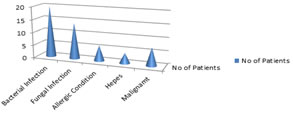
Figure 1: Study of vagino – vulvular disorder in the age group 16-24
TABLE 2: Study of Vagino-Vulvar disorders in different age groups of 25-45 years. (Total No.ofpatients-42)
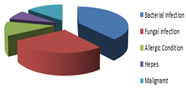
Figure 2: Study of vagino-vaginal disorders in the age group of 25-45 years
TABLE 3 : Study of Vagino-Vulvular disorders age groups of 46-66 year (Total No.ofpatients-51)
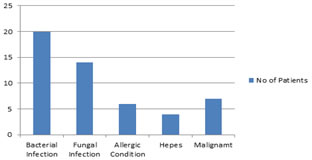
Figure 3: Study of Vagino-Vulvular disorders in the age group of 46-66 years.
DISCUSSION The present study of vaginal, vulvar disorders in Malayalam population in different age group. In the age groups between 16-24. The total number of patients were 3211(34.3%) had Bacterial infection, 9(28.1%) Fungal infection, 7(21.8%) had Allergic disorder,3(9.37%)had Herpes, 2(6.25%) had Malignancy. (Table-1) In the age group between 25-45 years the total number of patients were 42, 15(35.7%) had bacterial infection, 13(30.9%) Fungal infection, 6(14.2%) Allergic disorders, 5(11.9%) Herpes, 3(7.1%) had Malignancy. (Table-2) The patient aged between 46-66 years the total number of patients were 51, 20(39.2%) had Bacterial infection, 14(27.4%) had Fungal infection, 6(11.7%) had Allergic disorders, 4(7.84%) had Herpes, 7(13.7%). (Table-3) These findings were more or less in agreement with previous studies.6,7,8 Bacterial infection includes Bacterial vaginosis, Human Papilloma virus, Molluscumcontagiosum, Trichomoniosis, Scabies and Atrophy of vaginalvulvular. Fungal infections due to vulvo vaginal candidiasis caused by Candida albicans quite comman in all age groups9Malignancy was higher in 46-66 age group (13.7%). Allergic condition was higher in 16-24 ahe group(21.8%) could be usage of soap, detergents, medications which irritate the vulva vaginal and allergic contact dermatitis too Herpes hiquest in 25-45 age group (11.9%) is most comman cause of vulvar ulcer, these are 2 sereo type of HSV1 and HSV2more commonly associated with genital outbreaks. It is associated with pyrexia, dysuria, burning and pruritis. Vesicles are seen on the vulva which are more painful often found on cluster patient was severe pain with retention of urine. Malignancy of vulva can be caused by human papilloma virus (HPV) and Bartholin glands which are lubricating glands may from cyst.This cyst may develop into malignancy. In addition to this psoriasis seborric dermatitis, squamous cell carcinoma, TeneaCruris, Lichen sclerosis’s associated with immune disorders like alopecia, vitiligo and hypothyroidism10 The present disorders are quite prevalent in lower or middle socio economic status who were poorly educated (11) who were unaware of unhygienic diseases moreover such infections were also observed in the Indian Society where premarital or extra marital sexual contact was the history of patients, moreover BV, VVC, Trichomonas, Vaginalis was commonly observed in sexually active patients12. Apart from this BV was commonly observed in females who were in the usage of Intra uterine contraceptive devices (IUCD) which was associated with increased menstrual flow and irregular vaginal bleeding. In addition to this, miscarriage had a history of Bacterial infection. VVC observed in females whose husband had extra marital relation or female herself had extra marital or pre-marital relation. Atrophic vaginitis is common vaginal condition due to low estrogen states, such as menopause (natural or surgical), breast feeding and sometimes as a result of medications.
SUMMARY AND CONCLUSION The present study of vaginal vulvular disorders at different age group will be useful to Gynecologist, Pathologist to classify the higher incidence as per their age group .Although vagina is lined by stratified squamous non-Keratinized epithelium with abundant hair to combat with infection. Hence female medico-social workers, Clinicians, Gynecologist must create awareness of hygiene among Indian women because majority of them illiterate. But this study demands further genetic, hormonal, nutritional, embryological, histo-pathological studies because exact pathogenesis of vagino-vulvular disorders still un-clear.
REFERENCES
Policy for Articles with Open Access:
|
|

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.