 Home
Home
|
Table of Content - Volume 17 Issue 2 - February 2021
Study of management of diabetes in pregnancy in Telangana population
Vijaylakshmi Chirumamilla
Associate Professor, Department of Obstetrics and Gynaecology, Mediciti Institute of Medical Sciences Ghanpur Medchal-501401 Telangana, India. Email: drvijaylakshmi05@gmail.com
Abstract Background: The prevalence of diabetes increasing globally. The majority is GDM (Gestational Diabetes Mellitus) and type I, II diabetes in pregnancy has greater risk to both mother and foetus. Method: 80 diabetic pregnant women were studied with classifying First trimester pregnancy second trimester pregnancy and third trimester pregnancy – HbSA1C BUN1 TSH, Urine protein to creatinine ratio, USG, with different intervals to assess the viability and foetal umbilical Doppler for foetal movements. Results: 32 (40%) had pre-existing diabetes (type I II) 48 (60%) GDM, while 28 (35%) were multigravid, 52 (65%) prime gravid. The types of delivery were 51 (63.7%) had lower segment caesarean section, 29 (36.2%) had spontaneous vaginal delivery. The complication of foetus Neonates were more as compare to pre-existing diabetes than GDM patients. Conclusion: The present study of both types of diabetes in pregnancy will be useful to obstetrics and gynaecologist, radiologist, endocrinologist to treat such patient’s efficiently to prevent the risk for mother and foetus. Keywords: GDM, BUN, USG, HbSA1C, Umbilical Doppler, Foetus/Neonates.
INTRODUCTION Diabetes Mellitus is quite common disease in India and abroad due to lack of exercise, sedentary life style, fast food intake, urbanization, more life expectancy obesity females are more prone to diabetes as compared to males1,2. GDM is defined as carbohydrate intolerance resulting in hyperglycaemia of variable severity with onset or first recognition during pregnancy (3). Prevalence GDM was about 18 to 20 % in north India in 2004 and rapidly increasing due to sedentary life style4. Diabetes during pregnancy has adverse out come not only to the foetus/neonates but also for the mother. GDM also increase complication rate in mother foetus Indians are at higher risk of developing diabetes and their complications due to their ethnicity and genetic predisposition. Hence attempt was made to evaluate both GDM and pre-existing diabetic pregnant women and their foetus/neonates also.
MATERIAL AND METHOD Eighty (80) pregnant diabetes women regularly visiting obstetrics and Gynaecology department of Mediciti Institute of Medical Science Hospital Ghanpur, Medchal-501401 Telangana State were studied. Inclusive Criteria: Pre existing type-I or type-II Diabetes mellitus and gestation diabetes. Out of 80 pregnant DM women 28 were multi gravid, 52 were prime gravid selected for study. Exclusion Criteria: The patients associated with cardio-vascular disease, undergone cardiac surgery, HIV positive pregnant women were excluded from the study. Method: The post-diagnostic testing included. A – In first trimester pregnancy – Laboratory studies were HbA1C, BUN (Blood Urea Nitrogen) Sr. creatinine, TSH, Urine protein to creatinine ratio, Blood sugar levels. B – In the second trimester pregnancy – Laboratory test were Urine-protein to creatinine study in women with elevated value in first trimester is repeated HbA1C and Ultra Sonography. 1 – First trimester for assessment pregnancy dating (EDD) and viability. 2 – Second trimester to rule out anatomic sonogram at 18-20 weeks and Echo cardiogram of foetus haemoglobin of foetus in case of elevated maternal Glyco haemoglobin in first trimester. 3 – In the third trimester to assess the foetal size, every four weeks from 26-36 weeks in women with pre-existing diabetes and USG for assessment of foetal size at least once in a 36-37 weeks for women with GDM. Apart from this, dietary therapy is to avoid single large meals and food with large percentage of simple carbohydrate and advised to take complex carbohydrate with cellulose. Insulin was given to achieve glucose profiles similar to non-Diabetic pregnant women and Glyburide and Metformin were also used although insulin is efficient and safety drug during pregnancy, quite effective and least harmful to foetus has been observed, although long term adverse effects are concerned. Foetal heart rate, foetal movements were assessed by USG and foetal umbilical Doppler. The duration of study was three years (July 2007 to August 2020) Statistical analysis: Various evaluations were classified with percentage. The statistical study was done SPSS software. This research paper was approved by Ethical Committee of mediciti Institute of Medical Science Ghanpur Medchal – 501401, Telangana.
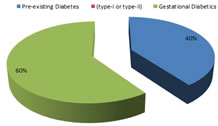
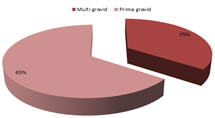
OBSERVATION AND RESULTS Table-1: Study of types of Diabetes in pregnant women 32 (40%) had pre-existing (type-I or type-II Diabetes), 48 (60%) had gestational diabetes. Table-2: Study of pregnancy in diabetes – 28 (35%) were multigravid, 52 (65%) were prima gravid. Table-3: Types of deliveries in diabetic women – 51 (63.7%) had lower segment caesarean section, 29 (36.2%) had spontaneous vaginal delivery. Table-4: Comparison of Neonate/ foetal complications in GDM and pre-existing Diabetes. Still births were 1 (1.25%0 in GDM and 3 (3.75%) in pre-existing Diabetes. Intra partum death were 1 (1.25%) in GDM and 2 (2.5%) in pre-existing diabetes. Shoulder dystocia was observed only in pre-existing diabetes 1 (1.25%0 Hydrocephalus was 1 (1.25%0 in GDM and 2 (2.5%) in pre-existing Diabetes. Congenital heart anomalies were 1 (1.25%) GDM, 3 (3.75%) in pre-existing diabetes, Marcosomia 1 (1.25%) in GDM and 2 (2.5%) in pre-existing diabetes. Jaundice was observed only in pre-existing diabetes 1 (1.25%). Table 1: Study of types of Diabetic in Pregnant women
Table 1: Study of types of Diabetic in Pregnant women
Table 2: Study of Pregnancy in Diabetics
Table 2: Study of Pregnancy in Diabetics
Table 3: Study of types of Deliveries in Diabetic women
Table 3: Study of types of Deliveries in Diabetic women
Table 4: Comparison of Neonatal foetal complication in GDM and pre existing Diabetes
DISCUSSION In present study the management of diabetes in pregnancy among Telangana Population. The pre-existing Diabetes (type-I, II) were 32 (40%) and 48 (60%) in gestational diabetes (Table-1). Types of pregnancy were 28 (35%) were multi gravid, 52 (65%) prima gravid (Table-2). The types of delivery were 51 (63.7%) had lower segment caesarean section, 29 (36.2%) had spontaneous vaginal delivery (Table-3), in the comparison of neo-natal or foetal complications in GDM and pre-existing diabetes. The more complication of foetus observed in pre-existing diabetes pregnancies (Table-4). These findings are more or less in agreement with previous studies5,6,7. In type-I Diabetes diagnosed during pregnancy most often present with unexpected coma. Early pregnancy may provoke diet and glycaemia control instability in patients with occult diabetes. Though it is rare but life threatening (8), but in type-II D. M. mother experiences double risk of serious injury at birth, triple the likelihood of caesarean delivery and need to be admitted at NICU (Newborn intensive care unit). Gestational diabetes accounts 90% of cases of pregnancy while pre-existing type-2 accounts for 8% if cases9. It was also observed that, increased risk of diabetic embryopathy leads to anencephaly, microcephaly and congenital heart disease and even spontaneous abortion. Hence there must be regular follow up in elevation in HbA1C values10. Diabetic management in pregnancy HbA1C, thyroid stimulation hormone, creatinine, urine albumin to creatinine ratio testing, review of medication list for potentially teratogenic drugs (i.e. ACE inhibitors, statins). It may also cause intra-uterine fatal demise neonatal hypoglycaemia and neonatal hyper bilirubinemia11. It is established fact that in hyperglycemias the blood has more viscosity. This viscosity retards or affects the proper blood flow hence there will not be suffice blood flow in micro and macro circulation of blood which causes multiple patho-physiological hazards as mentioned earlier (Table-5). Moreover hyperglycaemic blood mainly act upon cardio-vascular (maternal) and growing foetus and meticulous and regular check of blood glucose is necessary to prevent the morbidity and morbidity in both mother and foetus.
SUMMARY AND CONCLUSION Present study of management of Diabetic in pregnancy among Telangana population. The HbA1C level was remarkably high in pre-existing diabetes group rather than GDM group. As insulin is a drug of choice in diabetic pregnancy, which reduce the both maternal and foetal complications. Hence insulin administration is advised for such patients. But this study demands further nutritional, genetic, hormonal study because exact mechanism of insulin crossing placenta barrier is still unclear.
REFERENCES
Policy for Articles with Open Access
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.