 Home
Home
|
Table of Content - Volume 18 Issue 2 - May 2021
Placenta percreta: A rare case report
Manjusha Kale1*, Arati Mane2, Kranti Kendre3
1Junior Resident, 2Associate Professor, 3Professor, Department of Obstetrics and Gynaecology, MIMSR Medical College, Vishwanathpuram, Latur, Maharashtra 413512 Email: manjushakale1493@gmail.com
Abstract Background: Placenta Percreta, a rare complication of pregnancy, is associated with significant postpartum hemorrhage often requiring emergency hysterectomy. Majority of these cases are seen in patients with history of previous LSCS with anterior low-lying placenta. Here we present a rare case of Placenta Percreta which was diagnosed in a woman who was taken for emergency LSCS. Keywords: Placenta Percreta, Subtotal hysterectomy, LSCS.
INTRODUCTION Placenta percreta, the rarest and most severe form of placenta accrete spectrum, occurs when placenta extend through the entire myometrial layers and uterine serosa. The overall incidence of placenta percreta is extremely low with an incidence of 1 in 21000 pregnancies and majority of these cases are seen in patients with history of previous LSCS with anterior low lying placenta. The fundus of the uterus has thick myometrial lining and is seldom or almost never involved in percreta unless there is an history of fundal surgery in the past. Here we present the case of placenta percreta which presented as an obstetric emergency.
CASE REPORT A 34 years, 3rd gravida with 34 weeks amenorrhea, housewife from Latur was brought with c/o Bleeding per vaginum since morning (6 hours) and pain in abdomen since 2 hours. Patient was asymptomatic till morning, when she noticed spotting per vaginum, sudden onset, painless and causeless with one pad being partially soaked and stopped on its own after one hour. She then experienced 2nd episode of bleeding which was more than previous bleeding, but this time, she also had pain in abdomen, colicky type confined to lower abdomen and radiating towards thighs. Pain was relieved on its own temporarily reappearing after 30 minutes, so she visited nearby PHC after which she was referred to us. History of Present Pregnancy Spontaneous conception. 1st trimester – uneventful (1st scan normal); 2nd trimester- uneventful (2nd scan normal). No h/o bleeding, HTN, GDM, trauma. 3rd trimester – 3rd scan at 28 weeks s/o – low lying placenta 2 cm away from os and one cervical fibroid of 3*3 cm (risk was explained) Last scan done one-week back s/o- 33-34 weeks maturity with placenta previa 1.5 cm away from os with breech and a cervical fibroid of 3*4 cm. Menstrual History Regular/28 days cycle/bleeding 4-5 days/ average/ not associated with pain. LMP- 20/4/20 Obstetric History G3P1L1A1 Married since 8 years G1: FTND, 7 years female child G2: MTP; conceived due to contraception failure. G3: Present Pregnancy
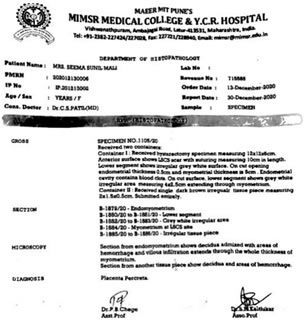
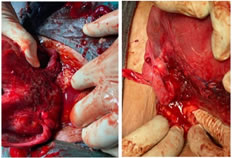
Past History: H/o laparoscopic surgery (cystectomy) done for Left ovarian cyst (chocolate cyst) Family History: Not significant General examination: Conscious, oriented. Pulse rate- 90 beats/min, RR- 16/ min, BP- 110/80 mm Hg Systemic examination: P/A - Fundal height 34 weeks Breech presentation with Mild contractions FHS- 110/min, regular Non tender P/S- Bleeding present but cervix not visualize properly and a mass is seen. P/V- Not done. Provisional diagnosis: G3P1L1A1 with 34 weeks pregnancy with APH (placenta previa) with breech presentation with cervical fibroid in preterm labour. Differential diagnosis: Placenta Previa or Abruption Investigations: CBC- Hb-9.3, TLC-14600, PLT-197000; BT-3min, CT-4:30 sec BSL-78.9, RFT- BUN-10.6, sr. creat-0.54 LFT- Sr.protein – 6.3, albumin- 3.0, globulin- 3.3, sr. total bilirubin- 0.40, direct bilirubin- 0.19 SGOT-20, SGPT-14.7, Alk. Phosphatase- 121 Urine R/M- Albumin- nil, sugar- nil. In view of Ante Partum Bleeding and preterm labour, she was taken for Emergency LSCS. Operative Notes: Baby ddelivered. Placenta and membranes expelled out spontaneously. Uterus was closed in layers and it was found that both the ovaries were stuck to posterior uterine wall (Kissing ovaries) with ruptured chocolate cyst. Continuous bleeding present on posterior wall of uterus, uterus became atonic, Inj. Carboprost and Inj. Methargin were given; but bleeding was not controlled neither uterine tone was regained. Systemic devascularization done but still bleeding was not controlled and uterine tone was not regained. All uterine sutures were removed. Posterior wall was observed from inside, which revealed a rent connecting from inside out and tissues were resembling with placental tissues, suspicious of Placenta Percreta or Infective Endometriosis. Patient was landed in atonic PPH, so the decision of obstetric Hysterectomy was taken as a life saving measure. Specimen was sent for Histopathology report which suggestive of placenta percreta.
Figure 1
Figure 2
REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Pediatrics (Print ISSN: 2579-0897) (Online ISSN: 2636-4662) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.