 Home
Home
|
Table of Content - Volume 20 Issue 2 - November 2021
Effect of diabetes mellitus on menopause in women of Kolkata, West Bengal
Sunil Chakrabarti1, Anindya Roy2, Moulik Debnath3, Shafaque Anjum4, Enakshi Ghosh5*
1Consultant Gynaecologist, Avinash Dutta, Maternity Home, Kolkata, INDIA. 2Associate Professor and Head of the Department, Department of Physiology, Raiganj Government Medical College, Raiganj, Uttar Dinajpur, W.B, INDIA. 3Assistant Professor, 4Junior Resident (2nd. Year), 5Associate Professor, Department of Anatomy, R.G Kar Medical College, Kolkata, INDIA. Email: drenakshighosh@gmail.com
Abstract Background: This is a cross sectional study in women population with diabetes mellitus attending endocrine out patients department of SSKM Hospital (IPGME and R), to find out effects of diabetes on female reproductive system. Age of menopause is inversely related to duration of diabetes. Follicular stimulating hormone (FSH) and Luteinising hormone (LH) showed increased values in all women with Type-2 DM when compared with control population. Estradiol level is slightly lower but testosterone levels are persistently low in all diabetic women with abnormal menstrual symptoms. Keywords: Type 2 Diabetes mellitus, Menopause, Estradiol level, Testosterone level.
INTRODUCTION Menopause is clinically manifested as absence of menstrual period for more than one year at the end of reproductive age. Gradual reduction in number of primary follicles present in ovary takes place from the age of 30 years. Blood estradiol level is also reduced with reduction in number of follicles. Pituitary gonadotrophin hormones steadily rise (FSH and LH) due to negative feedback action of oestrogen. Menopause is a process that occurs over a period of five to ten years. It begins when a woman’s body slows down its production of oestrogen and progesterone, the hormones responsible for ovulation and menstrual periods become irregular and eventually cease. The average age for most women to have their last period is 51, although the process can begin any time from the age 40 to the late fifties. The hormonal fluctuations that characterize menopause may have effect on blood glucose control. Diminished progesterone may have greater insulin sensitivity, but with less oestrogen can also cause increased insulin resistance. Lack of these hormones can also cause other changes which can worsen diabetic complications. For example, lowered oestrogen levels increase the risks of cardiovascular disease, which is already higher for people who have diabetes, and osteoporosis. Some symptoms of menopause could be confused with signs of hypoglycaemia and hyperglycaemia, such as dizziness, sweating and irritability. Metabolic changes that occur with menopause may contribute to the development of diabetes, including increased central body fat, insulin resistance and low-density lipoprotein cholesterol, and decreased high-density lipoprotein cholesterol levels (Carr 2003). Szmuilowicz et al. (2009) suggested that although weight gain commonly occurs during the menopausal transition, it is largely attributable to ageing. These changes in body composition have, in turn, been associated with alterations in insulin sensitivity and glucose metabolism, rendering women with type 2 diabetes at increased risk of cardiovascular disease (Perera et al. 2002). Ethical clearance has been taken from the intuitional ethical committee of IPGME andR, Kolkata, west Bengal.
Aims and Objectives
Sample Design: First stage was selection of patient who fulfilled inclusion and exclusion criteria. Next stage was to motivate the patient to participate with supply of informed consent in local language. In final stage, data was collected in the clinical data sheet. All columns filled up one by one in the diabetic clinic of SSKM hospital with the help of attending nursing personel. All documents related to her present and past diseases scrutinized and related information kept in clinical data sheet. Similarly, control patients were included from Uluberia S.D. Hospital, Howrah, after motivation and with their consent. The fasting blood sugar was estimated to exclude presence of diabetes. The informations were collected in the respective data sheets. Finally, blood samples were collected within first seven days of menstruation and sent to laboratory. Inclusion Criteria: Women with diabetes in reproductive age group. Post menopausal women with diabetes within five years of menopause. Age-matched women who did not have diabetes served as controls. Exclusion Criteria: Women with Type 1 diabetes. Women on oral contraceptive pill, hormone replacement therapy or, any other steroid hormone, oral or, inject able. Women with poorly controlled hyperglycaemia, in whom stoppage of oral anti-diabetic medication or, insulin for 48 hr (which was a pre-requisite for assay of serum insulin) was considered ethically unacceptable. Women with any significant chronic systemic illness like renal impairment (CHD Stage 3 or above) malignancy etc. where insulin therapy cannot be stopped temporarily. Sample Size: Sample size calculation was performed based on the primary objective of determining effect of diabetes on female reproductive system. This sample size included both urban and rural area attending diabetic clinic of SSKM Hospital, Kolkata,W.B. As previous studies showed large variation in urban and rural prevalence of diabetes (approx 10% and 4% respectively). Using a precision of 20% and allowing for a non response rate of 20%, total sample size was calculated 260. Institutional ethics committee clearance was obtained from IPGMER vide No, Inst/IEC/35 dated 03/01/2007. Written informed consent was obtained from respondents after ensuring that the subject understood her role in the study. Structured questionnaire was supplied and identification with anthropometric parameters was noted. TYPE OF STUDY: Observational. Data collection procedure: History taking, Tissue preparation of Ovaries including Uterus and blood sample collection.
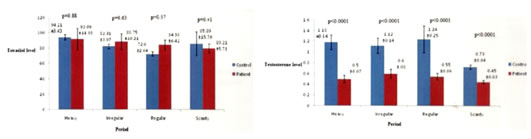
METHODOLOGY Sample of blood was collected in the early follicular phase of the cycle in empty stomach. Hormone estimation was done at the laboratory of Endocrine Department at IPGME and R by Chemo luminescence method. Particularly free testosterone and oestrogen, LH, FSH levels were measured from blood sample taken within first 10 days of menstruation of diabetic ladies in reproductive age group, in case of postmenopausal female, blood was collected on any date with informed consent from patient. Blood was collected for serum insulin estimation 48 hours after stoppage of anti-diabetic medicine and insulin injection, only if the clinical situations permit. The bar diagrams (figure 1, figure 2, figure 3, figure4) showing relations o0f FSH, LH. ESTRADIOL and TESTOSTERONE with different types of menstruation of diabetic women with control females.). Statistical Tools: Statistical analysis was done by SPSS version -17 using Unpaired and Paired ‘T test ‘and Pearson correlation test. P value less than .05 was taken as significant value. Figure 1 Figure 2 Figure 1: Relation of FSH with different types of menstruation in diabetic women with control females having similar symptoms; Figure 2: Relation of LH with different types of menstruation in diabetic women with control females having similar symptoms Figure 3 Figure 4 Figure 3: Relation of ESTRADIOL with different types of menstruation in diabetic women with control females having similar symptoms; Figure 4: Relation of Testosterone with different types of menstruation in diabetic women with control females having similar symptoms
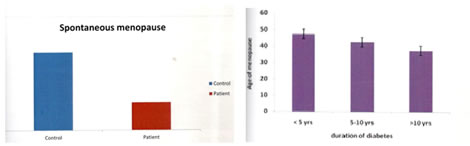
RESULTS Diabetes mellitus damage ovarian follicles in the same way as it damages other end organs like kidney, brain and heart. So, earlier loss of ovum result in lower age of menopause. Age of menopause is inversely related to duration of diabetes and glycosylated haemoglobin— (Hba1c) two well known factors responsible for end organ damage in diabetes mellitus. So we can say age of menopause is earlier in patients with diabetes mellitus (43 years vs. 47 years) than control population. Figure 5 Figure 6 Figure 5: Mean age of spontaneous menopause in diabetic women with control; Figure 6: Relation between age of menopause and duration of diabetes.
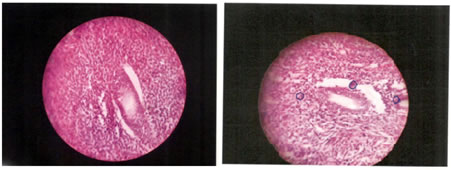
The main study shows reduced mean age of spontaneous menopause (43years) in diabetic women when compared with non diabetic control population (47years) moreover this is inversely proportional to duration of diabetes. The figures 5, 6 showing histopathology of ovaries of women having diabetes with normal females and also the histopathology of ovaries of women with long term uncontrolled diabetes in which the ovarian tissue show prominent apoptotic bodies in stromal tissue.
Figure 7 Figure 8 Figure 7: Histopathology of ovary in a woman (42) years, non diabetic; Figure 8: Histopathology of ovary in a woman of 42 years , having diabetes for 6 years , with Hba1c 9.5 showing prominent apoptotic bodies in stromal tissue with generalised follicular atrophy.
DISCUSSION Mean age of menopause in this study group is 43 years, lower than control population 47 years. Lower age of menopause in diabetes has been supported by several studies and there is a correlation between early onset of menopause and development of diabetes. Recent work have demonstrated effect of diabetes in follicular cells. Moreover age of menopause is inversely related to duration of diabetes, which is a known factor to develop complication in diabetes. Recent literatures have already analysed effect of hyperglycaemia in ovarian function. Possibly diabetes in the same way damages other end organs as it causes damage to the ovarian follicles and clinically expressed as earlier onset of spontaneous menopause.
CONCLUSION Diabetes mellitus damages ovarian follicles in the same way as it damages other end organs like kidney, Brain and Heart. So, earlier loss of ovum result in lower age of menopause. Age of menopause is inversely related to duration of diabetes and glycosylated haemoglobin—two well known factors responsible for end organ damage in diabetes mellitus.
REFERENCES
Policy for Articles with Open Access
|
|

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.