 Home
Home
|
Table of Content - Volume 21 Issue 1 - January 2022
Severe preeclampsia complicated by acute pulmonary oedema: Case report
Deepika Gulati1*, Soumyaa Agrawal2, Sudha Rani G3, Sriram Gopal4
1,2Junior Resident, 3Professor, 4Professor And H O D, Department of Obstetrics and Gynaecology, D Y Patil Hospital, Navi Mumbai, INDIA.
Abstract Background: Hypertensive disorder in pregnancy is one of the supreme causes of maternal mortality according to World Health Organization. Preeclampsia is a multiorgan disease characterized by new onset development of hypertension and proteinuria after 20 weeks. Acute pulmonary oedema in pregnancy is a rare complication but a life-threatening condition. Our case report focuses on importance of identifying the risk factors, early diagnosis of the complication and active management. A 36-year-old, G2P1L1 35 weeks of gestation, a known case of preeclampsia on anti-hypertensive drugs presented with dyspnoea, desaturation and BP of 190/110 mm hg. Chest x-ray s/o pulmonary oedema. BP stabilisation done along with management of pulmonary oedema with anti-hypertensives, diuretics and non-invasive ventilation. LSCS performed and patient shifted to ICU. Post op period uneventful. Keywords: preeclampsia, pulmonary oedema.
INTRODUCTION Preeclampsia is a multiorgan disease characterized by new onset development of hypertension and proteinuria after 20 weeks. It is characterized by increased systemic vasoconstriction and peripheral vascular resistance with defects in capillary permeability. Acute pulmonary oedema in pregnancy is a rare complication but life-threatening condition. Aetiology includes decreased colloid osmotic pressure, increased hydrostatic pressure and increased capillary permeability which results in extravasation of fluid from the vasculature. Timely diagnosis and management of pulmonary oedema is important to prevent maternal and foetal morbidities and mortality. We report a case of 36 yr. old G2P1L1 35 weeks gestation with Severe preeclampsia complicated by acute pulmonary oedema.
CASE REPORT A 36-year-old G2P1L1 previous FTVD 35 weeks gestation referred from outside hospital with complained of acute onset of breathlessness. She was recently diagnosed with Preeclampsia on tablet labetalol 100 mg TDS. On arrival in casualty, she was conscious and oriented with blood pressure of 190 /110 mm Hg. No complaints of premonitory symptoms, chest pain, fever, cough. No history of h/o bronchial asthma, tuberculosis, ischemic heart disease, URTI, inhalation/ingestion of toxic substance. On examination she had pulse of 108/min with 88% saturation at room air and RR of 24/minute with abdominal and pedal edema. On auscultation Bilateral basal Crepitations heard. S1 S2 normal. No murmurs. On per abdomen examination IUGR noted. Uterus was 30 weeks, relaxed with FHR 142/minute and on per vaginum closed cervix noted On USG OBS examination the baby had FGR type 2 with EFW of 1.7 kgs and doppler suggestive of utero-placental insufficiency. USG abdomen showed normal liver echotexture. Chest x-ray revealed pulmonary edema in bilateral lower zone with moderate pleural effusion. ECG showed Sinus tachycardia.2 D echo was normal. No valvopathy. Ejection Fraction was more than 60%. Covid Rapid Antigen test was negative. Liver enzymes SGOT and SGPT were raised up to 180u/L and 220u/L with normal bilirubin. Urine routine revealed proteinuria +3. RFT and coagulation profile were normal.
DIAGNOSIS: ACUTE PULMONARY OEDEMA SECONDARY TO SEVERE PREECLAMPSIA. MANAGEMENT: Tab nifedipine 10 mg given orally to the patient and Oxygen started at 8 lit/min via NRB mask. Injection Furosemide given intra venously with antibiotics. Decision was taken to deliver the baby by caesarean section in view of Severe Preeclampsia and IUGR with unfavorable cervix. Injection MgSO4 was given according to Zuspan regimen. Intra operatively mild ascites seen with thin meconium stained liquor. A male baby weighing 1650 grams delivered and shifted to NICU. Use of Inj. oxytocin was restricted during delivery. Post operatively patient was shifted to ICU. Covid RTPCR report came negative. Care was taken to maintain Negative Balance and avoid unnecessary use of Intra venous fluids. Patient improved dramatically after 24 hours of delivery with maintenance of saturation at room air. Injection Furosemide was continued for 48 hours after delivery. Pulmonary Oedema resolved on post LSCS chest X-ray. She was maintained on Tab Nicardia 10 mg BD with incentive spirometry. Repeat SGOT and SGPT were normal. Patient got discharged on post-operative day 6 and was counselled to do regular follow up till 6 weeks.
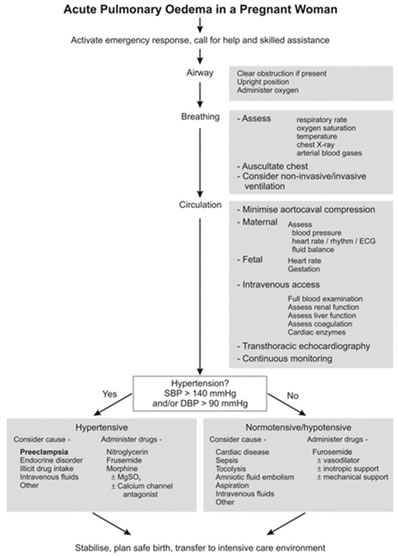
Following figure provide intervention modalities for pregnant patient with pulmonary oedema4 Figure 1
DISCUSSION Criteria1 for Severe preeclampsia includes: Blood pressure of more than and equal to 160 mm hg systolic or more than or equal to 110 mm Hg diastolic recorded on at least two occasion 4 hours apart, thrombocytopenia less than 100,00*109 /L. Renal insufficiency (serum creatinine more than 1.1mg/dl). Pulmonary edema. New onset headache unresponsive to medication. Visual disturbances. Acute Pulmonary edema is predisposed by an increase in capillary permeability, or an increase in intravascular hydrostatic pressure with increase in systemic vascular resistance and hypovolemia which leads to extravasation of fluid from the vasculature to alveolar spaces.2 In a study done by Sibai, severe preeclamptic-eclamptic patients had pulmonary oedema for an incidence of 2.9%. Risk factors reported were increased maternal age and multi gravida.3 Other Risk factors include pre-existing cardiac disease, sepsis, multiple gestation, injudicious use of intra venous fluids, magnesium sulphate toxicity and tocolytic agents like isoxsuprine.
CONCLUSION Acute pulmonary oedema is an emergency which require prompt treatment to prevent catastrophic effects for mother and fetus. Patient should also be explained about risk of developing cardio vascular diseases later in life and they should be monitored for the same. Transthoracic echocardiography is used in differentiating a low cardiac output from a high cardiac output condition along with other causes of acute pulmonary oedema.5
REFERENCES
zx
Policy for Articles with Open Access
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.