 Home
Home
|
Table of Content - Volume 21 Issue 2 - February 2022
Prevalence of maternal thrombocytopenia and anaemia in pregnant woman - An institutional experience
K Madhuri1, Naimisha Movva2*
1,2Associate Professor, Department of Obstetrics and Gynaecology, Mamata Medical College and General Hospital, Khammam, Telangana, INDIA. Email: mamatakhmm@gmail.com
Abstract Background: Thrombocytopenia and Anaemia in pregnancy is an important cause of maternal and perinatal morbidity and mortality hence need to pay a serious attention in pregnant woman and to be treated as soon as possible to prevent serious outcomes associated with these disorders. Hence the present study was aimed to determine the prevalence of gestational thrombocytopaenia and anemia among pregnant women. Materials and Methods: This was a cross sectional study from 110 pregnant women attending the outpatient department and wards of Department of Obstetrics and Gynaecology for a period of 9 months. Blood sample (random) was collected for peripheral blood film and haemoglobin count to evaluate platelet and haemoglobin levels. Results: The mean age of pregnant woman was 24.58 ±3.65 years. Most of the study subjects are from rural residence and were employed by occupation and in 2nd trimester of pregnancy. The prevalence of anaemia and thrombocytopenia in this study was found to be 67% and 19% respectively. Conclusion: Thrombocytopenia and anemia are a serious alarm for both mother and the baby, screening for platelet and haemoglobin count, and health educations, nutrition assessment, are needed during antenatal care. Keywords: Anemia; Thrombocytopenia; Pregnancy; platelet and haemoglobin.
INTRODUCTION Platelets are non-nucleated cells derived from megakaryocytes in the bone marrow and normally live in the peripheral circulation for as long as 10 days. Platelets play a critical initiating role in the haemostatic system.1 It is well documented that, in pregnancy, one of the important hematologic abnormality second to anaemia is thrombocytopaenia. The diversity of factors causing thrombocytopenia includes gestational thrombocytopenia, idiopathic thrombocytopenic purpura or preeclampsia.2 Other causes include infection, such as malaria or folate deficiency, and diseases, such as leukemia and aplastic anemia which may leads to considerable morbidity and mortality.3 Gestational thrombocytopenia is considered to be simply a modest exaggeration of the normal drop in blood platelets that commonly occurs in pregnancy. It is known that pregnant women with thrombocytopenia have a higher risk of bleeding excessively during or after childbirth, particularly if they need to have a cesarean section or other surgical intervention during pregnancy or labor. Such bleeding complications are more likely when the platelet count is less than normal range.4 Anaemia in pregnancy was recognized as unpleasant effects on the mother and a major public health problem in India leading to low birth-weight and high infant mortality. Anemia may be defined as a hemoglobin level below the 5th percentile of a trimester-specific hemoglobin reference level in iron supplemented women.5 The cause of anemia during pregnancy is multifactorial and includes nutritional deficiencies of iron, folate, and vitamin B12 and also parasitic diseases, such as malaria and intestinal parasitic infections.6Iron deficiency anemia is commonly associated with thrombocytosis, although severe thrombocytopenia has been reported in rare cases. Thrombocytopenia and anemia during pregnancy has become a cause for unnecessary, often invasive, additional testing and cesarean deliveries. The cause of gestational thrombocytopaenia is unclear, although it might be secondary to accelerated platelet consumption and the increased plasma volume associated with pregnancy.7 This study was designed to determine the prevalence of gestational thrombocytopaenia and anemia among pregnant women reporting for antenatal care at our tertiary healthcare centre.
MATERIAL AND METHODS Subjects: This was a cross sectional study from 110 pregnant women attending the outpatient department and wards of Department of Obstetrics and Gynaecology of Mamata General and Super Speciality Hospital, Khammam, Telangana, from July 2020 to March 2021. This study was approved by the Institutional ethical committee. Duly signed Informed consent forms were collected from all the participants during the study. A detailed history and physical examination were carried out for every subject who entered in the study as per a pre-designed proforma. Pregnant women with the following conditions were excluded from the study: Bleeding disorders, Women on non-steroidal anti-inflammatory drugs such as aspirin, Splenomegaly, Connective tissue disease such as SLE, Hypertension, HIV and hepatitis B infection. Information such as drug history, presence of splenomegaly and HIV / hepatitis B status were extracted from the clinical notes. Specimen: A total of 3 ml of blood sample (random) was taken from each pregnant woman for peripheral blood film and complete blood count. Complete blood count was determined using a BeneSphera H33s automated haematology analyzer. Haemoglobin in the blood was estimated by the method of Drabkin and Austin (1932). Quality control was determined on a daily basis by analysis of three different manufacturer-provided samples with known cell counts. A pregnant woman was considered anaemic if haemoglobin was <11 g/dl. Severity of anaemia was measured as follows: mild if Hb was 9.0–10.9 g/dl; moderate if Hb was 7.0–8.9 g/dl; and severe if Hb was <7.0 g/dl. Thrombocytopenia is said to be present when the platelet count of the pregnant women is less than 150 × 109 / L. The platelet counts from 100 to 150 × 109/L is considered mild thrombocytopenia, levels ranging from 50 to 100 × 109/L are considered as moderate thrombocytopenia and levels less than 50 × 109/L are considered as severe thrombocytopenia Statistical analysis: Data analysis was done by using SPSS Package version. Simple proportions, mean, standard deviation and Student “t” test and Chi-square test was used to find out the association between two groups. P value of less than 0.05 is considered as statistically significant.
RESULTS In this study, the maximum number of pregnant woman 71 % were of age 31-40 years and 21% of the woman belongs to 21-30 years and remaining 10% were of above 40 years. The mean age of the study participants were 24.58 (±3.65) years. Most of the study subjects 65% lived in a rural residence. Among the study subjects, 68% were housewife and 42% were employed by occupation. Among the study subjects, 58% were illiterates. The gestational age of the woman showed 47% of them were in 2nd trimester. (Table 1) Table 1: Sociodemographic characteristics of pregnant women (N = 110)
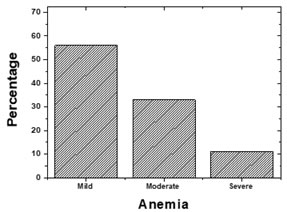
Figure 1: Prevalence of Anaemia among Pregnant Women
The prevalence of anaemia in this study was found in 74 (67%) pregnant women, the remaining 36 (33%) women had RBC count in the normal range. Among the 74 anaemic pregnant women in this study the prevalence of anaemia was mild in 56%, 33% moderate, and 11% severe anaemia, Figure 1. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

Variables |
Thrombocytopenia (%) |
Anaemic (%) |
|
Age group (years) |
21– 30 |
3 (14) |
14 (19) |
31–40 |
16 (76) |
54 (73) |
|
≥ 40 |
2 (10) |
6 (8) |
|
Occupation |
Housewife |
15 (71) |
55 (74) |
Employed |
6 (29) |
19 (26) |
|
Educational status |
Illiterate |
12 (57) |
54 (73) |
Literate |
9 (43) |
20 (27) |
|
Residence |
Rural |
10 (48) |
62 (84) |
Urban |
11 (52) |
12 (16) |
|
Trimester |
1st trimester |
14 (67) |
56 (76) |
2nd trimester |
5 (24) |
12 (16) |
|
3rd trimester |
2 (10) |
6 (8) |
|
Women of age group 31-40 years had higher prevalence of anaemia (73%) and thrombocytopenia (76%) than other age groups; whereas, women with employment had lower prevalence anemia (26%) and thrombocytopenia (29%) but the difference was not statistically significant. Other factors that were analysed with anaemia during pregnancy include education, residence, and gestational age where most of the pregnant woman has shown anemia and thrombocytopenia in 1st trimester and were of rural background (Table 2).
DISCUSSION
Thrombocytopenia and Anaemia in pregnancy was recognized as a major public health problem in India leading to a variety of physiologic or pathologic conditions, several of which are unique to pregnancy resulting in high maternal morbidity and mortality.8 It is the second commonest hematologic disorder, following anaemia in pregnancy. Women with thrombocytopenia in pregnancy have a higher tendency to bleed; postpartum haemorrhage is a major cause of maternal mortality. This study was conducted in order to determine the prevalence of thrombocytopenia and anemia among pregnant women attending our hospital. In this study, the prevalence of thrombocytopenia and anemia among pregnant women was 19% and 67% respectively. Which was almost comparable to the results of studies conducted by earlier studies.7,9In developing countries, the cause of anemia during pregnancy is multifactorial and includes nutritional deficiencies of iron, folate, and vitamin B12 and also parasitic diseases, such as malaria and intestinal parasitic infections. The relative contribution of each of these factors to anemia during pregnancy varies greatly by geographical location, season, and dietary practice.10 In this study, the maximum number of pregnant woman was of age 31-40 years with mean age 24.58 years. From our findings, gestational thrombocytopenia occurred across the three trimesters. No case of severe thrombocytopenia was seen in first trimester. In the study, maximum cases (47%) of thrombocytopenia were seen in 2nd trimester weeks of gestation. This was in accordance with the report of Pandey and Singh who reported that gestational thrombocytopenia in pregnancy develops primarily in the late second trimester.7 Education has been reported to reduce the risk of being anaemic in several studies. Women who had education were less likely to be anaemic compared to their counterparts. Educated pregnant women have better income and eat nutritious food and hence do not get nutritional anaemia.11 Among the study subjects, 58% were illiterates. These results are in accordance with earlier study, reported that higher prevalence of anaemia among pregnant women who had no education.9,12 Secondary and higher education had been associated with several other good maternal and child outcomes. This study showed a significant association between anemia and rural residence, which is consistent with previous reports. In summary, thrombocytopenia and anemia are the crucial problems among pregnant women. The pregnant women in the present study were from a rural residence and illiterates and housewives, hence screening of pregnant women for platelet and haemoglobin count, and health educations, nutrition assessment, are needed during antenatal care. Hence Thrombocytopenia and anemia are a serious alarm for both mother and the baby and needs to be dealt on priority basis.
REFERENCES
- Katke RD, Gohil DP. Thrombocytopenia during pregnancy: an institutional based study. Int J Reprod Contracept Obstet Gynecol. 2014;3(4):947-51.
- Cines DB, Levine LD. Thrombocytopenia in pregnancy. Hematology 2014, the American Society of Hematology Education Program Book. 2017 Dec 8;2017(1):144-51.
- Gauer R, Braun MM. Thrombocytopenia. American family physician. 2012 Mar 15;85(6):612-22.
- Arnold DM. Bleeding complications in immune thrombocytopenia. Hematology 2014, the American Society of Hematology Education Program Book. 2015 Dec 5;2015(1):237-42.
- Sifakis S, Pharmakides G. Anemia in pregnancy. Annals of the New York Academy of Sciences. 2000 Apr;900(1):125-36.
- Allen LH. Anemia and iron deficiency: effects on pregnancy outcome. The American journal of clinical nutrition. 2000 May 1;71(5):1280S-4S.
- Pandey A, Singh R. Thrombocytopenia during pregnancy: an institutional based prospective study of one year. International Journal of Research in Medical Sciences. 2017 Aug;5(8):3502.
- Steer PJ. Maternal hemoglobin concentration and birth weight. The American journal of clinical nutrition. 2000 May 1;71(5):1285S-7S.
- Asrie F, Enawgaw B, Getaneh Z. Prevalence of thrombocytopenia among pregnant women attending antenatal care service at Gondar University Teaching Hospital in 2014, northwest Ethiopia. Journal of blood medicine. 2017;8:61.
- Vieth JT, Lane DR. Anemia. Emergency Medicine Clinics. 2014 Aug 1;32(3):613-28.
- Melku M, Addis Z, Alem M, Enawgaw B. Prevalence and predictors of maternal anemia during pregnancy in Gondar, Northwest Ethiopia: an institutional based cross-sectional study. Anemia. 2014 Oct;2014.
- Adam I, Khamis AH, Elbashir MI. Prevalence and risk factors for anaemia in pregnant women of eastern Sudan. Transactions of the Royal Society of Tropical Medicine and Hygiene. 2005 Oct 1;99(10):739-43.
Policy for Articles with Open Access
Authors who publish with MedPulse International Journal of Anesthesiology (Print ISSN:2579-0900) (Online ISSN: 2636-4654) agree to the following terms:
Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal.
Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.