 Home
Home
|
Table of Content - Volume 18 Issue 3 - June 2021
A study of low-level laser therapy for treatment of androgenic alopecia
Shankar Rangrao Sawant
Associate Professor, Department of Dermatology, Vedantaa Institute of Medical Sciences, At Saswand Village, Post Dhundalwadi, Tahsil Dahanu District Palghar, INDIA. Email: drshankarsawant@gmail.com
Abstract Background: Alopecia is the most commonly observed disorder in dermatology. Androgenic alopecia is the most commonly observed alopecia. Alopecia has important effect on quality of life of a person. LLLT is a new invention for treatment of alopecia. Aim and objective: To study the low-level Laser therapy for treatment of androgenic alopecia Material and methods: Present study was a prospective experimental study carried out on patients with active androgenic alopecia. Total 30 Patients were treated using a device containing a combination of a medical laser device and a low-level light irradiation device, composed of 21 LDs (wavelength, 655±5 nm; mean output, 1.094 mW) and 30 LEDs (wavelength, 655±20 nm; output, 1.75 mW). Patients were followed up at 8 weeks and 16 weeks and Global photography and a phototrichogram were performed and results were noted. Results: Use of LLLT showed significant increase in Hair density at 8 weeks and 16 weeks (p<0.05). Significant increase in mean thickness of hair at 8 weeks (64.21± 22.3µm) and 16 weeks (69.6 ± 21.7 µm) as compared to baseline (62.21± 21.4 µm) was observed.
INTRODUCTION Alopecia is the partial or complete loss of hair especially on the scalp. Different types of alopecia exists but androgenic alopecia is the most common type of alopecia. 1 Androgenic Alopecia is seen in approximately 51% of the total number of males above age of 40 years and females who are above the age of 65 years and above. 2 Shankar DK et al. done a population based study of 1005 subjects in India and found 58% prevalence of AGA in males aged 30-50 years.3 Androgenic alopecia is also known as male pattern hair loss (MPHL) in males and female pattern hair loss (FPHL) in females. Androgenetic alopecia (AGA) is characterized by miniaturization of the hair follicle, resulting from alteration in the hair cycle dynamics, leading to vellus transformation of terminal hair follicle. In AGA, the duration of anagen phase gradually decreases and duration of telogen phase increases. Duration of anagen phase determines the hair length, the maximum length of the new anagen hair becomes shorter than that of its predecessor, leading to miniaturization and bald appearance.4,5 Etiological factors for androgenic alopecia includes hyperandrogenism, genetic inheritance, local scalp vasoconstriction and hypoxia.6 Various treatment modalities are available for treatment of androgenic alopecia. Medical management includes use of finasteride and minoxidil. These medicines have some contraindications for use and are associated with some side effects. Hair transplant is another modality used for treatment but is costly. Low Level Laser Therapy (LLLT) is an important invention in the treatment of androgenic alopecia. LLLT produces scalp vasodilation, increase ATP production and determine a modulation of reactive oxygen species and inflammatory mediators.7-9 Laser phototherapy stimulates the epidermal stem cells from the follicle bulge and generates shift from talogen to anagen phase. 10 LLLT induces and prolongs the duration of anagen and prevents a premature catagen phase of the hair cycle. 11,12 Laser therapy reverses hair miniaturization and an increased number of hairs per follicular unit. 13 LLLT also increases shaft diameter and decreases vellus hairs.14 Hair is an important part of human appearance. Hair loss lead to decreased quality of life. 15 LLLT can be an effective and less expensive treatment for alopecia so present study was conducted to see the effect of LLLT in the treatment of androgenic alopecia. Aim and objective: To study the low level Laser therapy for treatment of androgenic alopecia
MATERIAL AND METHODS Present study was a prospective experimental study carried out in department of dermatology at tertiary health care centre. Study population was patients visiting to OPD of department of dermatology with diagnosis of active androgenic alopecia. Inclusion criteria: 1. Patients with active androgenic alopecia (Ludwig classification of I to II for females and Norwood-Hamilton classification of II (IIa) to V for male) 2. Patients in age group of 19- 65 years 3. Patients willing to participate in the study Exclusion criteria: 1. Patients with other diseases of the hair and scalp (eg, dermatitis, psoriasis, infection, scalp injury) 2. Patient who previously received hair transplantation, hair weave, or scalp 3. Patients with chronic diseases or having photosensitivity 4. Patients taking other drugs for the symptoms 5. Patients who used hair dye 6. Pregnant and lactating females Study was approved by ethical committee of the institute. A valid written consent was taken from the patients after explaining study to them. Data was collected with pre tested questionnaire. Data included sociodemographic data like age, sex etc. Detailed clinical history was noted. Through clinical examination was done. After considering inclusion and exclusion criteria total 30 patients were studied. At first visit, Global photography and a phototrichogram were performed. Patients were treated using a device containing a combination of a medical laser device and a low-level light irradiation device, composed of 21 LDs (wavelength, 655±5 nm; mean output, 1.094 mW) and 30 LEDs (wavelength, 655±20 nm; output, 1.75 mW). At the start of study, tattooing was done with blue dye at central point of vertex as a reference point for measurement. The device was applied to hair for 25 minutes on alternate day for 16 weeks. Patients were followed up at 0, 8 weeks and 16 weeks and Global photography and a phototrichogram were performed and results were noted. Phototrichogram assessment was done using a medical device (dpHarris Scalp and Hair Diagnosis System; Chowis company, Yongin-si, Gyeonggi-do, Republic of Korea) at baseline, 8 weeks, and 16 weeks. Measurements were performed through a × 50 magnification lens. Hair density (hairs/ cm2) and the mean thickness (mm) of terminal hair were assessed by the clinical investigator at the tattooed region of each patient. Data was entered in excel sheet and analysed with SPSS version 22.0.
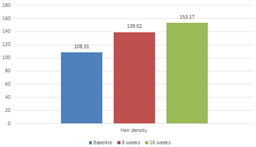
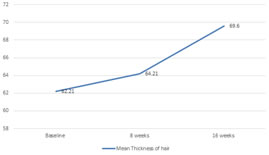
RESULTS We studied 30 patients. In our study, majority of the patients were from the age group of 41-50 years (36.67%). Followed by 51-60 years (23.33%). Patients in the age group of 19-30 years and 31-40 years were 16.67% each. Patients above the age group of 60 years were 6.66%. Mean age of the patients was 46.38± 7.3 years. Fig 1 shows distribution of patients according to gender. In our study, 11(63.33%) patients were male and 11(36.67%) were females. Male to female ratio was 1.72:1. We followed up the patients at 8 weeks and 16 weeks. Mean Hair density at baseline in all patients was 108.31± 35.3 hairs/cm2. Mean hair density at 8 weeks was 139.02± 37.5 hairs/cm2. At 16 weeks it increased upto 153.17± 35.6 hairs/cm2. Statistical analysis showed significant increase in Hair density at 8 weeks and 16 weeks (p<0.05). Fig 3 shows comparison of mean thickness of hair at baseline, 8 weeks and 16 weeks. Baseline mean thickness of hair was 62.21± 21.4 µm. Mean thickness of hair increased over follow up at 8 weeks and 16 weeks. Mean thickness of hair at 8 weeks was 64.21± 22.3µm at 8 weeks and 69.6 ± 21.7 µm at 16 weeks. On analysis significant increase in mean thickness of hair was observed (p<0.05).
Table 1: Distribution of patients according to age group
Figure 1: Distribution of patients according to gender
Figure 2: Comparison of mean hair density at baseline, 8 wks and 16 wks
Figure 3: Comparison of mean thickness of hair at baseline, 8 wks and 16 wks DISCUSSION In our study, Mean Hair density at baseline in all patients was 108.31± 35.3 hairs/cm2. Mean hair density at 8 weeks was 139.02± 37.5 hairs/cm2. At 16 weeks it increased upto 153.17± 35.6 hairs/cm2. Statistical analysis showed significant increase in Hair density at 8 weeks and 16 weeks (p<0.05). In our study we found significant increase in mean thickness of hair at 8 weeks (64.21± 22.3µm) and 16 weeks (69.6 ± 21.7 µm) as compared to baseline (62.21± 21.4 µm). Similar findings were seen in previous studies. Satino et al. studied 28 male and 7 females with androgenic alopecia. Patients were treated with HairMax LaserComb® 655 nm for 6 months for 5-10 minutes every day and found that greater results were seen in hair tensile strength in vertex area for males and temporal area for females.16 Leavitt et al. used The HairMax LaserComb® device in a double-blind, sham devicecontrolled, multicenter, 26-week trial randomized study among 110 male AGA patients. Patients used the device three times per week for 15 minutes for a total of 26 weeks . Significantly greater increase in mean terminal hair density compared to subjects in the sham device group has been reported.12 In a study by Kim S S et al., they studied 24 male with active androgenic alopecia and found that with use of low level laser therapy, increase in hair density on both the vertex (145.1/cm2 vs. 137.3/cm2 P < 0.005) and occiput (163.3/cm2 vs. 153.3/cm2, P < 0.005) and 83% of the patients reported to be satisfied with the treatment.17 In a study by Lanzafame et al., they treated patients with androgenic alopecia with a helmet helmet containing 21, 5 mW lasers and 30 LEDs (655±5 nm, 67.3 J/cm2, 25 minutes ) every other day for 16 weeks and found 35% increase in hair growth. 14 Kim et al. found that Even though mean hair thickness (12.6±9.4 vs. 3.9±7.3 in control group, P = 0.01) hair density (17.2±12.1 vs. –2.1±18.3 in control group, P = .003) increased significantly in the treatment group, there was no prominent difference in global appearance between the two groups.18 Similar results were observed by Avram and Rogers et al. where they found LLLT increased hair count and shaft diameter.13
CONCLUSION Low Level Laser Therapy is effective in treatment of androgenic alopecia in terms of increased hair thickness and increased hair density
REFERENCES
Policy for Articles with Open Access
|
|

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.