 Home
Home
|
Table of Content - Volume 21 Issue 2 - February 2022
A study of clinical profile of patients with cardiomyopathy
Jinaga Satyanarayan Rao1, P Ratnachary2*
1,2Associate Professor, Department of General Medicine, Kamineni Academy of Medical Sciences, Lb Nagar, Hyderabad 500068 Telangana, INDIA. Email: rcpanuganti@gmail.com
Abstract Background: Prevalence of cardiomyopathy is increasing all over the world. Various factors are responsible for development of cardiomyopathy Aim And Objective: To study the clinical profile of patients with cardiomyopathy Material And Methods: Present study was a prospective study carried out on patients admitted with symptoms and signs cardiomyopathy. Data collected was sociodemographic data, clinical history and clinical examination. All patients underwent echocardiography, ECG and chest radiography. Results: Most common type of cardiomyoipathy is Dilated cardiomyopathy (87.5%) followed by Hypertrophic cardiomyopathy (10%) and Restrictive cardiomyopathy (2.5%). Biventricular failure was the most common clinical presentation followed by left heart failure and then right heart failure.
INTRODUCTION Cardiomyopathy is a primary disorder of the heart muscle that causes abnormal myocardial performance and is not the result of disease or dysfunction of other cardiac structures. They are distinctive because they are not the result of pericardial, valvular, hypertensive or congenital diseases.1 The incidence of DCM is reported to be 5 to 8 cases per 1,00,000 population per year. It occurs 3 times more frequently in males as compared to females. It is also more common in blacks.2 There are several classifications of cardiomyopathy based on etiology, gross anatomy, histology, genetics, hemodynamic function, etc. The most useful classification is however the one based on etiology. Commonly cardiomyopathies are classified according to pathology in functions as dilated cardiomyopathy, hypertrophic cardiomyopathy and restrictive cardiomyopathy. Cardiomyopathies are associated with ventricular and valvular dysfunction. Important investigations in diagnosis of cardiomyopathy are detailed clinical examination, electrocardiogram, chest X-ray and a two-dimensional echocardiogram with Doppler flow. Cardiomyopathies are treated according to cause and symptoms of the patients. Various studies were conducted on etiology, pathophysiology, clinical presentation, evaluations and management of cardiomyopathy. Most of these studies are conducted considering one type of cardiomyopathy at a time, present study was conducted to know the clinical profile of all types of cardiomyopathies. Aim and objective: To study the clinical profile of patients with cardiomyopathy.
MATERIAL AND METHODS Present study was a prospective study carried out in department of Medicine at a tertiary health care centre. Study population was patients admitted with symptoms and signs cardiomyopathy Inclusion criteria: 1. Patients with symptoms and signs of heart failure (dyspnea, palpitation, PND, orthopnea, pedal edema, chest pain, cough, easy fatigability) 2. Patients with ECHO findings Left ventricular ejection fraction <45%, Left ventricular end diastolic dimension > 3 cm / body surface area, Global hyokinesia and Dilatation of all the chambers of heart. Exclusion criteria: 1. Patients with Valvular heart disease, Congenital heart disease and pericardial disease 2. Patients with Cor. pulmonale with CHF. 3. Patients with Hypertension 4. Patients not willing to participate in the study Study was approved by ethical committee of the institute. A valid written consent was taken from the patients after explaining study to them. Data was collected with pre tested questionnaire. Data included sociodemographic data, clinical history and clinical examination. All patients underwent echocardiography, ECG and chest radiography. The echocardiographic criteria were based on the recommendations of the American society of echocardiography and American heart association. Patients with past history of myocardial infarction or coronary angiography showing significant luminal occlusion (>70%) were diagnosed as ischemic cardiomyopathy. Peripartum cardiomyopathy was diagnosed based on the criteria laid down by Demakis and colleagues which includes Development of cardiac failure in the last month of pregnancy or within 5 months of delivery. Diabetic cardiomyopathy was diagnosed with prolonged DM of more than 10 years and alcoholic cardiomyopathy was diagnosed with patients with H/O alcoholism. Idiopathic cardiomyopathy was diagnosed with no obvious cause. Data was entered in excel sheet and analysed with SPSS version 20.0
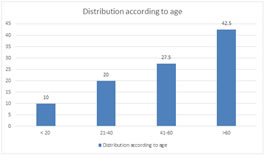
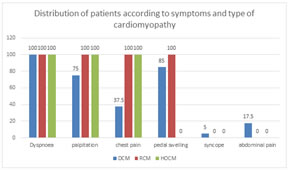
RESULTS We studied 40 patients. Majority of the patients were above the age of 60 years followed by 41-60 years (27.5%). Patients in the age group of 21-40 years were 20%. Patients below the age of 20 years were 10%. (fig 1) Out of 40 patients, 25 (62.5%) were male and 15 (37.5%) were female. Male to female ratio was 1.67:1. In our study, 87.5% patients had dilated cardiomyopathy 35(87.5%). Hypertrophic cardiomyopathy and restrictive cardiomyopathy were seen in 10% and 2.5% patients respectively. (table 1) Most commonly observed risk factor in our study was coronary artery disease 13(32.5%). Diabetes mellitus and alcoholism was seen in 22.5% patients each. Hypertension was observed in 5(20%) individuals. Peripartum cardiomyopathy was seen in 5(12.5%) patients. Other risk factors were thyroid disorders, neuromuscular disorders which were seen in 5 patients. Out of 40 patients, 4 patients did not have any risk factor. (table 2) Fig 2 shows Distribution of patients according to symptoms and type of cardiomyopathy. All the patients complained of dyspnoea. Palpitation was seen in all patients of RCM and HOCM. 75% patients with dilated cardiomyopathy had palpitation. Chest pain was seen in all patients of RCM and HOCM and 37.5% patients of dilated cardiomyopathy. Pedal swelling was seen in 85% patients of dilated cardiomyopathy and all patients of RCM. Syncope and abdominal pain was seen in 5% and 17.5% patients of dilated cardiomyopathy respectively. Table 3 shows Distribution of cardiomyopathy patients according to signs seen in patients. Most commonly observed sign was basal crepitation seen in 31(77.5%) patients. JVP was raised in 75% patients. Other signs were edema (70%), gallop (70%), systolic blood pressure below 100 mmHg (27.5%), hepatomegaly (37.5%) and ascites (20%). In our study, chest X ray shows 38(95%) patients had cardiomegaly. Out of total 40 patients, 33(82.5%) shows pulmonary congestion and 9(22.5%) shows pleural effusion. In our study, ECHO findings showed that 37(92.5%) patients with cardiomyopathy had mitral regurgitation and 31(77.5%) had tricuspid regurgitation. Aortic regurgitation was seen in 4(10%) patients. Diastolic dysfunction was seen in 18(45%) individuals. Other findings on ECHO were pericardial effusion (25%), pulmonary hypertension (22.5%). Global hypokinesia was seen in all patients. The mean LV ejection fraction was 32.51±6.56. The mean LV end diastolic diameter was 60.23± 4.28mm. The mean LV end systolic diameter was 47.4±6.1 mm. On ECG, majority of the patients had normal axis. Left axis deviation was seen in 19 (47.5%) patients. LAD was seen in 18 patients of dilated cardiomyopathy and 1 patient of HOCM. Right axis deviation was seen in 2(5%) patients. most commonly observed abnormalities were LBBB 17(42.5%) followed by VPC 8(20%). Other abnormalities were LVH 13(32.5%), RBBB 4(10%), atrial fibrillation 10(25%) and non specific ST changes 7(17.5%). HOCM patients showed non specific ST changes in one patient and LBBB in one patient. One patient with RCM had atrial fibrillation.
Figure 1: Distribution of cardiomyopathy patients according to age
Table 1: Distribution of patients according to cardiomyopathy
Table 2: Distribution of cardiomyopathy patients according to risk factors
Figure 2: Distribution of patients according to symptoms and type of cardiomyopathy
Table 3: Distribution of cardiomyopathy patients according to signs
DISCUSSION In our study, Majority of the patients were above the age of 60 years followed by 41-60 years (27.5%). Out of 40 patients, 25 (62.5%) were male and 15 (37.5%) were female. Male to female ratio was 1.67:1. Ahmed et al. 3 in 2005 studied 100 patients, and observed that the mean age was 52.9 ± 15.1 years in males and 51.3.9±17.7 years in females. Teple et al. studied all types of cardiomyopathy, they found 76.1% were male, 24.9% were females with mean age of 45.16 13 years.4 In our study, 87.5% patients had dilated cardiomyopathy 35(87.5%). Hypertrophic cardiomyopathy and restrictive cardiomyopathy were seen in 10% and 2.5% patients respectively. Similarly, in a study by Patil VC et al., DCM was seen in 72.3% patients. HOCM and RCM in 16.92% and 7.69% patients respectively.5 Most commonly observed risk factor in our study was coronary artery disease 13(32.5%). Diabetes mellitus and alcoholism was seen in 22.5% patients each. Hypertension was observed in 5(20%) individuals. Peripartum cardiomyopathy was seen in 5(12.5%) patients. In a study by Parale et al. 75% patients had no risk factors. Peripartum cardiomyopathy was seen in 12.5% patients. Other risk factors were diabetes (7.5%) and alcoholism (5%).6 Most commonly observed symptom in our study was dyspnoea and palpitations. Chest pain was seen in all patients of RCM and HOCM and 37.5% patients of dilated cardiomyopathy. Pedal swelling was seen in 85% patients of dilated cardiomyopathy and all patients of RCM. Similar findings were seen in Hoskatti et al. where they found dyspnoea (100%), pedal edema (70%), palpitation (56.6%), chest pain (40%), abdominal pain (33.3%) and syncope (16.6%).7 Most commonly observed sign was basal crepitation seen in 31(77.5%) patients. JVP was raised in 75% patients. Other signs were edema (70%), gallop (70%), systolic blood pressure below 100 mmHg (27.5%), hepatomegaly (37.5%) and ascites (20%). Similar results were observed in Hoskatti et al., and Ahmed et al. (3,7) In our study, chest X ray shows 38(95%) patients had cardiomegaly. Out of total 40 patients, 33(82.5%) shows pulmonary congestion and 9(22.5%) shows pleural effusion. Similar findings were observed in previous studies. NM Ammash, James B. Seward and et al., study on RCM, observed that, most common presenting complaint was dyspnea (71%) followed by pedal swelling (46%), palpitations (33%), fatigue (32%), orthopnea (22%) and chest pain (22%).8 In a study by Sheriff M. Helmy, Gomaa F. Maauof and et al. on HOCM, 21 patients were presented with chest pain, 15 had palpitations, 15 with shortness of breath and 5 with syncope, 9 patients were asymptomatic.9 In our study, ECHO findings showed that 37(92.5%) patients with cardiomyopathy had mitral regurgitation and 31(77.5%) had tricuspid regurgitation. Aortic regurgitation was seen in 4(10%) patients. previous studies show lesser prevalence of MR than our study,10,11 this was due to large proportion of patients with ischemic dilated cardiomyopathy and severe LV dysfunction compared to non ischemic cardiomyopathy. In our study, Left axis deviation was seen in 19 (47.5%) patients. Right axis deviation was seen in 2(5%) patients. Teple et al. observed 33.3% patients had LAD and 4.8% patients had RAD. Most commonly observed abnormalities were LBBB 17(42.5%) followed by VPC 8(20%). In Teple et al., LBBB and RBBB were seen in 9.5% patients each.4 Other abnormalities in our study were LVH 13(32.5%), RBBB 4(10%), atrial fibrillation 10(25%) and non specific ST changes 7(17.5%). Teple et al. found non specific ST-T changes in 42.9% patients. 4
CONCLUSION Dilated cardiomyopathy was most common cardiomyopathy with signs of heart failure.
REFERENCES
Policy for Articles with Open Access
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.