 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 11 Issue 2 - August 2019
Optic disc drusen or true papilledema - A diagnostic dilemma
Vandna Sharma1*, Rajeev Tuli2, Gaurav Sharma3, Mandeep Tomar4
1,2,3,4Department of Ophthalmology, Dr RPGMC, Tanda, Kangra, Himachal Pradesh, INDIA. Email: drrajeevtuli@gmail.com, drgaurav.sharma@gmail.com, sunnyigmc85@gmail.com, vandna.27@rediffmail.com
Abstract Optic nerve head drusen (ONHD) are calcified deposits which are either buried or at the surface of optic disc1. Buried drusen are often found in younger age and can obscure optic disc margins. The optic disc can appear to have no "optic cup", resulting in the appearance of papilledema2. A clinical case in which the optic nerve head is severely swollen is easy to diagnose as true papilledema but if, it appears to be mildly or moderately elevated, associated with symptoms of headache, with no other signs or symptoms of raised intracranial pressure (ICP), the diagnosis becomes more challenging3,4. Thus, the diagnostic dilemma begins with making the clinical decision and answering the question, “is it or is it not swollen?” It is important to differentiate between ONHD and true swelling of the optic nerve head as one has to take decision who will be referred for urgent neurological assessment and who can be monitored routinely. We present here two cases which were earlier diagnosed as bilateral papilledema but on further evaluation with the help of current imaging techniques, revealed that the true cause of disc elevation was ONHD and thus dilemma was solved. Key Word: true papilledema.
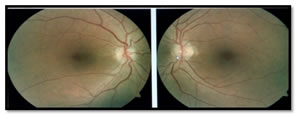
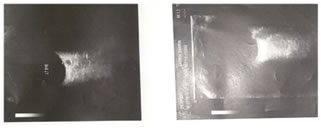
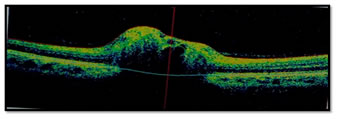
INTRODUCTION Optic nerve head drusen (ONHD) are calcified deposits which are either buried or at the surface of optic disc1. Buried drusen are often found in younger age and can obscure optic disc margins. The optic disc can appear to have no "optic cup", resulting in the appearance of papilledema2. A clinical case in which the optic nerve head is severely swollen is easy to diagnose as true papilledema but if, it appears to be mildly or moderately elevated, associated with symptoms of headache, with no other signs or symptoms of raised intracranial pressure (ICP), the diagnosis becomes more challenging3,4. Thus, the diagnostic dilemma begins with making the clinical decision and answering the question, “is it or is it not swollen?” It is important to differentiate between ONHD and true swelling of the optic nerve head as one has to take decision who will be referred for urgent neurological assessment and who can be monitored routinely. Effective management of these disc elevations will reduce over-referrals for neurological evaluations, thus avoiding needless and expensive neurological testing and decreasing health care costs 5.We present here two cases which were earlier diagnosed as bilateral papilledema but on further evaluation with the help of current imaging techniques, revealed that the true cause of disc elevation was ONHD and thus dilemma was solved. CASE 1 A 45 year old female, initially presented to her local physician with the complaint of headache since two years. She was suspected for bilateral papilledema and underwent further neurological evaluation. Her CT scan was done to exclude intracranial space occupying lesion (ICSOL), which found to be normal. The possibility of idiopathic intracranial hypertension (IIH) was considered as a cause of papilledema. So, she was started on medication (tab.-acetazolamide 250 mg) and kept on follow up for two years. It was observed that papilledema was not resolving. So, she was referred to an ophthalmologist for further evaluation. She was also complaining of diminution of vision for distant in both eyes (B/E). Her retinoscopy was done and correction was given. Her dilated fundus examination revealed bilateral small, hyperaemic, elevated optic discs with "lumpy-bumpy" appearance, blurred margin, absent optic cup, and with no surrounding retinal oedema or any vascular abnormalities, so the possibility of optic disc drusen was kept (Figure1). Rest of the ocular examination was normal including intraocular pressure (IOP) and visual fields. B-scan ultrasonography revealed highly reflective round structures in B/E (Figure2). To further confirm the diagnosis, spectral domain optical coherence tomography (SD-OCT) was done. It showed the bilateral elevation of discs with lumpy-bumpy internal contour and abrupt decline in the subretinal hyporeflective space (SHYPS). Retinal nerve fibre layer (RNFL) thickness was normal, with absent “lazy V” pattern which ruled out presence of papilledema on SD-OCT (Figure3).
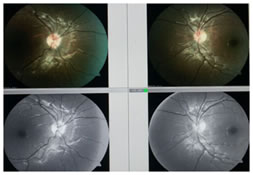
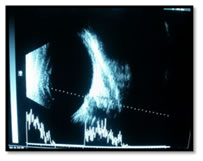
CASE 2 An 11 years old female presented with headache from last one year. Her retinoscopy was done and found to be within normal limits. Her dilated fundus examination revealed bilateral small, hyperaemic, elevated discs with ill defined margins, with no cup and normal peripapillary area (Figure 4). Rest of ocular examination was normal. B-scan ultrasonography revealed highly reflective round structures in both eyes suggestive of disc drusen (Figure 5). SD-OCT showed elevation of disc with irregular internal contour, abrupt decline in SHYPS thickness and normal RNFL thickness (Figure 6).
Figure 3: SD-OCT image of ONH of case 1- showing irregular internal contour
Figure 5: B-Scan of second case Figure 6-SD-OCT image of ONH showing “lumpy-bumpy” internal contour, with an abrupt decline in the subretinal hyporeflective space suggestive of optic nerve head Drusen and normal RNFL thickness. DISCUSSION Optic nerve head drusen (ONHD) are acellular deposits of calcium, nucleic and amino acids, and mucopolysaccharides.6,7,8 There are two main types of ONHD: visible drusen and "buried" drusen. Visible drusen are located near the surface, can be visualized with help of direct ophthalmoscope. Due to these superficial drusen ONH has typically an irregular lumpy-bumpy appearance9. With the age these superficial drusen become visible because of drusen growth or the neural tissue loss obscuring these drusen. In contrast, if drusen are deeply located in the disc nearer to the lamina, they can be quite difficult to detect. In such cases imaging techniques may be needed for confirmatory diagnosis.10,11,12 ONHD are estimated to occur in 0.3% of the population, with both genders affected equally.13,14 In approximately 75% of cases, drusen are bilateral, with a higher chances of occurrence in the nasal rather than temporal optic disc sectors.9,15 It has been proposed that underlying cause of development of disc drusen might be abnormal axonal metabolism resulting in abnormal deposition of calcium crystals in mitochondria, extrusion of mitochondria into the extracellular space with disruption of axons and further accumulation of calcified cellular contents 1. Although ONHD are normally asymptomatic, but they can be related to visual field defects, seen in 24%–87% of affected adults.9,10,12 The drusen-associated visual field loss may be due to mechanical stress on delicate structures within the prelaminar scleral canal.8 The visual field defects of ONHD ranges from defects similar to that seen in glaucomatous optic neuropathy to defect showing enlargement of blind spot1. Predisposition to acute vascular events, such as retinal artery occlusion, retinal vein occlusion, and anterior ischemic optic neuropathy is there due to impaired blood flow leading to congested optic disc secondary to ONHD8. Rarely, central vision is affected if subretinal choroidal neovascularisation is present. The ONHD are usually an independent finding, but can be associated with other conditions, such as pseudoxanthoma elasticum (PXE), retinitis pigmentosa, and angioid streaks2.The current diagnostic techniques including B scan ultrasonography, fundus fluorescein angiography (FFA), a computed tomography (CT) of the orbits are useful to diagnose the ONHD. Ultrasound B scan shows hyper-reflective echo and on the CT- hyper-dense lesion at the optic nerve head suggestive of drusen16. On SD-OCT, ONHD generally have a “lumpy-bumpy” internal contour with an abrupt decline in the SHYPS in contrast to this in true papilledema there is smooth internal contour and the SHYPS is thickest near the optic nerve head followed by a gradual tapering away from the optic disc forming a “lazy V” pattern17. To diagnose and confirm pseudopapilledema in case of buried optic nerve head drusen (ONHD) which are often misdiagnosed as true papilledema, often poses a diagnostic dilemma. In these scenarios, a confirmatory test to document the ONHD can be helpful and prevent unnecessary invasive investigations and prolonged unwarranted costly treatment.
CONCLUSION Optic nerve head elevation results from a number of aetiologies which can be broadly divided into two groups: pseudopapilledema (looking like papilledema but not true papilloedema) and true swelling, such as occurs in papilledema due to raised intracranial pressure5. If medical history, clear signs/symptoms associated with optic disc oedema, and a thorough eye examination are not pointing to a definitive diagnosis, then FFA, B-scan ultrasonography and SD-OCT are adjunctive tests which can be helpful in precisely assessing and/or quantify the disc and retinal nerve fibre layer features5. Differentially diagnosing between pseudopapilledema and true swelling of the optic nerve head is an important task for ophthalmic practitioners as it will further decide the management of the patient either urgent neurological assessment or routine monitoring1.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.