 Home
Home
|
Table of Content - Volume 14 Issue 2 - May 2020
A prospective study of etiological analysis on optic disc edema cases
Shaloo Negi1, Rajeev Tuli2*, Rattan Kumar Sharma3, Amit Bhardwaj4, Rajesh Sharma5
{1Resident, 2Professor & HOD, 3Professor, 5Resident, Department of Ophthalmology} {4Associate Professor, Department of Neurology} Dr Rajender Prasad Medical College, Kangra At Tanda. INDIA. Email: negi.shaloo@gmail.com
Abstract Background: Optic disc swelling is a pathological condition with a variety of causes. As the etiologies of optic disc edema are important from prognostic point of view, early recognition of its cause and prompt treatment is required. Aim: To investigate the etiologies in optic disc edema cases. Material and Methods: A total of 73 patients diagnosed with disc edema were investigated for causes. Thorough ophthalmic examination was performed and CT and MRI scans were also done. Results: Most common etiology of disc edema was idiopathic intracranial hypertension (IIH), which was observed in 30.13% of the patients. Non-arteritic anterior ischemic optic neuropathy was observed in 19.18% and grade 4 hypertensive retinopathy was observed in 8.2%. Conclusion: Early recognition of optic disc edema, its cause and early treatment is important from prognostic point of view. The early detection and management are essential to prevent progress of disease and loss of vision. Keywords: optic disc edema, papilloedema, idiopathic intracranial hypertension, Non-arteritic anterior ischemic optic neuropathy
INTRODUCTION Optic disc swelling is a pathological condition with a variety of causes. The most common causes of optic nerve swelling are non-arteritic anterior ischemic optic neuropathy, optic neuritis and intracranial pathology. Unilateral optic disc swelling is more likely to be due to demyelinating optic neuritis, non-arteritic anterior ischemic optic neuropathy, retinal vein occlusion and diabetic papillopathy. Bilateral swelling is more likely to be due to papilledema, toxic optic neuropathy and malignant hypertension. Other causes include intracranial conditions such as tumor, cerebral trauma, intracerebral or subdural hemorrhage and lyme disease. Some medications have been associated with raised ICP, for example tetracycline, minocycline, lithium, isotretinoin, nalidixic acid and corticosteroids (both use and withdrawal).1 Vascular causes includes retinal vein occlusion, malignant hypertension and acute lymphocytic leukemia (through infiltration of retinal vessels by immature lymphocytes).1 As the etiologies of optic disc edema are important from prognostic point of view, early recognition of its cause and prompt treatment is required.2 Role of ophthalmologist is to monitor all parameters of optic nerve function for field assessment and fundus photograph to document the changes in disc. Thus, the present study was conducted to investigate the etiologies in optic disc edema cases.
MATERIAL AND METHODS Study design: Non randomized prospective case study Inclusion criteria: All the patients above 15 years of age. Patients presenting with unilateral or bilateral disc edema. Patients willing to participate in the study. Exclusion criteria: Patients with hazy media impairing the visualization of fundus. Patients not giving consent. Methodology: Prior permission of institutional ethics committee was obtained. Patients were registered and informed consent was taken from them for the study. Patients were evaluated with detailed history of symptoms including defective vision for distant and near, headache, double vision, transient visual-obscuration, nausea, vomiting, altered consciousness, deviation of eyeball to left or right along with their onset, duration and progression. In all patients were history of hypertension, diabetes mellitus and any other systemic illness, head injury, brain tumour, ocular infection was noted. Past history of ocular infection, surgery, trauma, history of any drugs use like amiodarone, tetracycline etc. were also noted. In female patients, obstetric history was taken carefully. Examination findings including general physical examination, pulse, blood pressure was done. Thorough ophthalmic examination was performed as under: Distant uncorrected visual acuity of all patients using Snellen’s chart or illiterate E chart of both eyes along with corrected visual acuity using pinhole. Pupil size and reaction. Relative afferent pupillary defect by swinging flash light examination. External eye examination for conditions like exophthalmos, buphtalmos, deviation of eyeball. Extraocular movements both for ductions and versions in all cardinal positions. Slit lamp examination to see any opacity in all media, anterior chamber depth, lens for evidence of cataract, pseudophakia, aphakia and anterior vitreous for pigment and cells. Color vision by Ishihara’s chart. Intraocular pressure with schiotz tonometer. Visual fields evaluation using automated perimetry with Humphrey 30-2 program. Dilatation of pupils with tropicamide 1% eye drops in patients with normal IOP and normal anterior chamber depth. Fundus evaluation using direct ophthalmoscope (Heine beta 200s) and +90D aspheric volk lens and Haag streit B M 900 slit lamp biomicroscope. Optic disc evaluation using +90D condensing lens was done and disc cup size, colour, cup disc ratio, cup disc asymmetry between two eyes, hyperaemia of disc, blurring of disc margins, forward protrusion of disc, haemorrhage over disc, tortuosity of vein and venous pulsation were noted. Fundus photography was done in all patients. Investigations including complete hemogram, serum lipid profile, thyroid test, chest x ray and cerebrospinal fluid analysis was done in specific cases. Magnetic resonance imaging and computerized tomography scan was done all patients.
RESULTS In the present study, a total of 73 patients were enrolled and there were 43 females and 30 males. Mean age of all patients in the present study was 39.7 ± 15.43 years. Most common age group was 21 to 40 years (54.8%), followed by 41 to 60 years (28.8%), more than 60 years (12.3%) and only 4.1% were aged less than 20 years. Bilateral involvement was seen in 61.6 % and unilateral involvement was found in 38.4% of patients. Table 1: Stages of papilledema (Modified Frisen scale classification)
Table 2: CT scan findings in patients with disc edema (N=73)
CT scan revealed mass effect in three patients, neurocysticercosis in two patients and arachnoid cyst, cerebral venous thrombosis of transverse sinus, fracture of sphenoid bone, hydrocephalous, interparenchymal hemorrhage, pituitary microadenoma, mucosal thickening in sphenoid sinus and contusion in temporal lobe in one patient each. Rest of the patients had an unremarkable CT scan.
Table 3: MRI scan findings in patients with disc edema (N=73)
MRI scan was normal in 78% of the patients. There were two patients of anaplastic astrocytoma, one patient each of cavernous sinus thrombosis with pachymeningitis, arachnoid cyst, contusion in frontal region, cerebral venous thrombosis of right transverse sinus, increased caliber of optic nerve, increased CSF in perioptic space, NCC, pilocytic astrocytoma with bleed, subfalcine herniation, tortous optic nerve, hydrocephalous and pituitary microadenoma.
Table 4: Aetiology of disc edema (N=73)
Most common etiology of disc edema was IIH, which was observed in 30.13% of the patients. NA-ION was observed in 19.18% and grade 4 hypertensive retinopathy was observed in 8.2%. Tubercular meningitis was observed in four patients. Posterior uveitis and space occupying lesions were observed in three patients each. Ethambutol induced ON was observed in two patients. Less common etiological causes observed in our patient population were AION, cavernous sinus thrombosis, cerebral venous thrombosis, CRVO, cryptococcal meningitis, diabetic papillopathy, head injury, IC Bleed, pitutary microadenoma, posterior scleritis and TON.
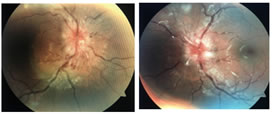
Images: (Right eye) (Left eye) Image 1: Polycythemia vera presented with stage IV papilledema (Frisen scale classification)
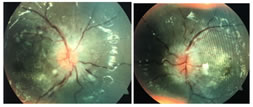
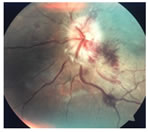
(Right eye) (Left eye) Image 2: Grade IV hypertensive retinopathy showing disc edema and macular star formation
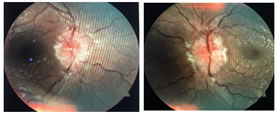
(Right eye) (Left eye) Image 3: Idiopathic intracranial hypertension showing stage IV papilledema
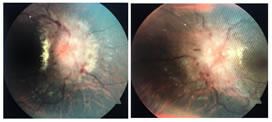
(Right eye) (Left eye) Image 4: Neurocysticercosis showing stage V papilledema
DISCUSSION In this study, staging was done according to modified Frisen scale classification.34,35 Stage II papilledema was noted in 2.3%, stage III was found in 23.3%, Stage IV was noted in 37.2% and stage V was found in 37.2% of patients. So, it was observed that, majority of the patients had established papilledema in our study. Most common etiology of optic disc edema in our study was idiopathic intracranial hypertension (IIH), which was observed in 30.13% of the patients. Non-arteritic anterior ischemic optic neuropathy (NAION) was observed in 19.18% of the patients and grade 4 hypertensive retinopathy was observed in 8.2% of patients. Less common etiology observed in our patient population were AION, cavernous sinus thrombosis, cerebral venous thrombosis, CRVO, cryptococcal meningitis, diabetic papillopathy, head injury, IC Bleed, pitutary microadenoma, posterior scleritis and TON. Ijima et al.3 conducted a study to investigate the etiology of bilateral disc swelling in Japanese population. In their study, the most common cause of the bilateral disc swelling was increased intracranial pressure (ICP) (59%), followed by pseudopapillitis (16%), uveitis (8%), hypertensive retinopathy (5%), bilateral optic neuritis, acute disseminated encephalomyelitis (ADEM) and optic disc drusen (all at 2% each), and leukemia (1%). Similar to our study, the observations in this study also reflect that increased ICP is the most common etiology observed in patients with optic disc edema. When attempting to diagnose the etiology of bilateral disc swelling, patients should be immediately examined for the possible influence of other diseases which increase intracranial pressure. Idiopathic intracranial hypertension (IIH) was observed in 30.13% of patients in our study. Out of 22 patients of IIH, 17 were females and 5 were males. Most common age group affected was between 21-40 years of age. In a study conducted by Rani et al.,4 most common cause of papilledema was idiopathic intracranial hypertension which was present in 24 patients (32%) in the age group of 30 to 40 years. IIH is a syndrome characterized by elevated intracranial pressure that usually occurs in obese women in the childbearing age group. The signs and symptoms of idiopathic intracranial hypertension are so subtle, that the patients maintain an alert and oriented mental state and has no localizing neurologic findings. Headache which is the usual presenting symptom of the patients with IIH was also the most commonly reported symptom in our patients (63%).5 Friedman et al.6 reviewed medical records of 82 patients with idiopathic intracranial hypertension (IIH) to determine the frequency of headaches occurring after initial diagnosis and treatment of IIH. They observed that patients with IIH frequently had other types of headaches, which were not necessarily related to increased intracranial pressure. In addition, other headache syndromes frequently coexist such as rebound headache from analgesic or caffeine overuse and require their own therapy. Non-arteritic anterior ischemic optic neuropathy (NAION) was observed in 19.18% of patients in our study. The most commonly affected age group was between 41- 60 years. Jung et al.1 also conducted a similar study to investigate the clinical manifestations and diagnoses of optic disc swelling in Korean patients. NA-AION was the most common cause of (34.7%) optic disc swelling in their study and the mean age of the patients with NA-AION was 53.4 years. In their study, many patients with NA-AION had other medical conditions (e.g., DM, hypertension, and hypercholesterolemia) also, which was the cause of higher rate of NA-AION diagnosed in older patients. This was consistent with our study findings, since most of the patients in our study also had similar comorbidities. Huaiyu et al.7 conducted a study to determine etiology of optic neuritis in patients of different ages in china. In their study, 44% of patients had idiopathic demyelinating Optic neuritis and 9.8% had findings suggestive of multiple sclerosis, most commonly in the age group of 16-45 years. Whereas in our study, six out of 73 patients (8.22%) had optic neuritis. Out of these six patients, two (3.3%) had findings suggestive of multiple sclerosis on MRI. This was most commonly seen in the age group of 21-40 years in our study. Ethambutol induced optic neuritis was observed in 4.1% of patients taking ethambutol in the dose of 25 mg/kg body weight (according to Fixed dose combination regime for TB 2017). Hong Kong's guideline on ocular toxicity of ethambutol, suggests that regular visual acuity test may be considered in patients with risk factors, especially with high dose (25mg/kg/day) or prolonged treatment with ethambutol. With the usual daily dosage of 15mg/kg/day for patients under the care of Tuberculosis and Chest Service in Hong Kong, incidence of ethambutol induced ocular toxicity is below 1%.8 In our study, 26% of the patients had hypertension out of which 8.22% of patients had grade IV hypertensive retinopathy and 9.6% of the patients were found to be diabetic, out of which one patient had diabetic papillopathy. In a retrospective study conducted by Bayraktar et al.9 on 3,235 patients with diabetes, diabetic papillopathy was diagnosed in 24 eyes (0.37%). Of those 24 cases, 50% were unilateral. They found that only 63% of the patients with diabetic papillopathy had diabetic retinopathy. Papilledema was present in 43 patients (58.9 %) in our study, most commonly in the age group of 21-40 years. Out of these 43 cases, 22 patients had IIH, six had grade IV hypertensive retinopathy, four had tubercular meningitis, three had space occupying lesion, two had NCC while cryptococcal meningitis, intracranial bleed, pituitary microadenoma, head injury, cavernous sinus thrombosis and cerebral sinus thrombosis was observed in one patient each. In a study conducted by Solanki et al.,10 70% of patients had papilledema most commonly in the age group of 21-30 years. In their study out of 35 patients with papilledema, twelve patients had space occupying lesion, six had meningitis, five had malignant hypertension, four had drug history, three had malaria and one patient each of diabetes, pseud tumor cerebri, anemia, and encephalopathy and head injury. Most common causes of space occupying lesion were superior sagittal sinus thrombosis, neoplastic growth in brain, posterior fossa tumor, and venous infarct in brain in their study. While in our study 4.11% of patients had anaplastic astrocytoma. Ijeri et a..11 also conducted a similar study on 43 cases of optic disc edema. They concluded that, out of 15 patients (34.9%) who had papilledema, six patients had meningitis, three had superior sagittal sinus thrombosis, one had intracerebral hemorrhage, one had subdural hematoma, one had grade IV hypertensive retinopathy and in three cases, the cause was unknown (idiopathic). Follow up of patients was done after 48 hours and no changes were observed in visual acuity, visual field and stages of papilledema in any of the patients after 48 hours of presentation. Patients presenting with severe headache should undergo complete ophthalmic examination. If papilledema is suspected, neuroimaging is necessary to rule out any intracranial mass. Patients with ICSOL may present with headache and diplopia. Patients with optic disc edema should be evaluated further based upon the history and examination. Unilateral disc edema due to local causes should be investigated and managed accordingly. Neuroimaging is recommended for unexplained optic disc edema (especially bilateral). Typically, the preferred imaging study is MRI of the brain and orbit with and without contrast. In emergency setting CT scan is preferred. If the MRI is negative, a lumbar puncture may be needed to assess for elevated opening pressure and signs of infection or inflammation (e.g., CSF cell count, protein and glucose). Laboratory or serologic testing is done if infectious etiology is suspected.
CONCLUSION Early recognition of optic disc edema, its cause and early treatment is important from prognostic point of view. If papilledema is detected later, it could lead to loss of vision. Hence, the early detection and management are essential to prevent progress of disease and loss of vision.
REFERENCES
Policy for Articles with Open Access
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.