 Home
Home
|
Table of Content - Volume 14 Issue 3 - June 2020
Dry eye in diabetics: Clinical study in rural population
Pallavi Bangalore Acharlu1*, Ramya R Nadig2, Sujatha Vijayalekshmi3, Vijay Kumar Srivastava4
1Assistant Professor,2Junior Resident, 3Professor, 4Professor and HOD, Department of Ophthalmology, MVJ Medical College and Research Hospital, Hoskote, Bangalore. Email: pallaviacharlu@gmail.com
Abstract Background: Diabetic Retinopathy, Cataract, Glaucoma, Keratopathy, Refractive changes, Cranial nerve palsy and Chronic inflammation of the Lids are complications associated with Diabetes. Dryness of eyes which is a common complaint is not given much importance. The aim of the study was to find distribution of dry eye in different grades of Diabetic Retinopathy in rural population. Methods: Our study is a hospital based cross-sectional study. A complete examination of anterior segment was done using slit lamp. Posterior segment was examined using Direct and Indirect Ophthalmolscope. Schirmer test and Tear break up time (TBUT) test was carried out in all participants. Results: 70 patients were included in our study .The prevalence of dry eye was 55.7%. in our study. Among 70 Diabetic patients, 50 (71.43%) patients had abnormal TBUT measurements. In our study dry eye showed significant correlation with increasing grades of Diabetic Retinopathy. Conclusion: Our study shows there is association between Dry eye and Diabetes and there is positive correlation with severity of Diabetic retinopathy Key words: Diabetes Mellitus, Diabetic Retinopathy, Dry eye, Schirmer Test, Tear break up time.
INTRODUCTION The common cause of blindness is Diabetes in people aged 20–70 years 1. Diabetic Retinopathy, Cataract, Glaucoma, Keratopathy, Refractive changes, Cranial nerve palsy and chronic inflammation of the Lids are complications associated with Diabetes 2. Recurrent corneal erosion, superficial punctate keratopathy, corneal endothelial damage and persistent epithelial defect are the keratopathies associated with Diabetes Mellitus. Apart from this, few of them have dry eye.2-5 According to few literature's diabetic patients have increased risk of developing corneal epithelial defects, reduced corneal sensitivity, abnormal wound healing, and increased susceptibility to infected corneal ulceration.6-10 The reported percentages of Ocular surface disorders and dry eye have been around 54%.11 Some other reports report a low prevalence of around 20% in type 2 Diabetic patients.12 There are very few studies done on dry eye in diabetics. The aim of the study was to find distribution of dry eye in different grades of Diabetic Retinopathy in rural population.
MATERIALS AND METHODS This study was conducted in Department of Ophthalmology in MVJ Medical College and Research Hospital from September 2019 to December 2019.It is hospital based cross sectional study. Informed consent was obtained. 140 eyes of 70 patients (Age: 40-70yrs) with Diabetes seeking routine ophthalmic checkup were included in the study. Individual who had corneal, conjunctival or ocular adnexal pathologies, systemic diseases with dry eyes, chronic ocular drug abuse, Ocular surgeries in the previous 6 months, Patients whose fundus was not visualized due to any media opacification and contact lens users were excluded from the study. Visual acuity, detailed slit lamp examination, Fundus exam by Direct and Indirect Ophthalmoscope was performed. Schirmer test and Tear break up time (TBUT) test was carried out in all participants. The patients were categorized into 5 groups according to the fundus finding as Group1 -No Diabetic Retinopathy, Group2-Mild Non Proliferative Diabetic Retinopathy (Mild NPDR), Group3- Moderate Non Proliferative Diabetic Retinopathy (Moderate NPDR), Group4-Severe Non Proliferative Diabetic Retinopathy (Severe NPDR) and Group5- Proliferative Diabetic Retinopathy (PDR). Schirmer test was performed using standardized Whatman filter paper without topical anesthesia. The strip was folded at 5mm and placed in the lower fornix at the junction of middle and lateral third of lid margin for 5 min. The amount of wetting of paper was measured in millimeter. The measurement >15mm was taken as Normal. Based on the Schirmer test readings Dry eye was Graded as follows: Mild Dry Eye 10-15 mm, Moderate Dry Eye 5-10mm, Severe Dry Eye <5mm. TBUT test was performed by staining the tear film using a fluorescein strip without using topical anesthesia and asking the patients to blink for few seconds to encourage its distribution. Cobalt blue filter was used to visualize the tear film without artificially holding the lids open. The time taken between the last blink and the appearance of the first corneal dry spot in the stained tear film was recorded. A TBUT value <10 s was considered abnormal.
STATISTICAL ANALYSIS Data collected was collated into MS Excel. Tables/ charts were generated using MS Excel. Qualitative variables are presented as percentages and continuous variables are presented as Mean± SD.
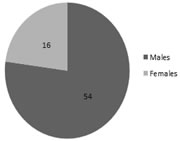
RESULTS 70 (140 eyes) Diabetic patients were included in our study. The mean (±standard deviation) age of Diabetic patients was 55.06 ± 9.70 years (Range 40 to 75 years). Out of 70 Diabetic patients 54 were Males (age 55.26 ± 9.62 years) and 16 were Females (age 54.38 ± 10.26 years). Table 1, Fig 1.
Table 1: Distribution of Age and gender in the study Groups
Figure1: Gender distribution of Diabetic Patients
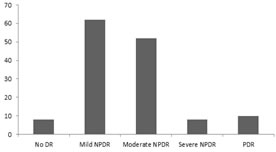
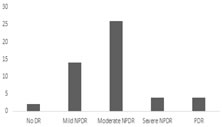
Among the Diabetic patients(140 Eyes), 8 eyes(5.7%) had No Diabetic Retinopathy, 62 eyes (44.28%) had Mild NPDR, 52 eyes(37.14) had Moderate NPDR, 8 eyes (5.7%) had Severe NPDR and 10 eyes(7.14%) had PDR(Fig 2). Figure 2: Distribution of Grades of Diabetic Retinopathy
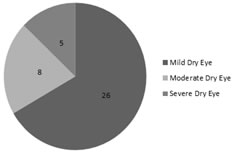
Among the 70 Diabetic Patients 39 patients (55.70%) had dry eyes. Mild dry eye was seen in 26 (52 eyes-37.14%) patients, Moderate dry eye was seen in 8(16 eyes-11.42%) patients and severe dry eye was seen in 5(10 eyes-7.14%) patients.(Fig 3).
Figure 3: Distribution of Grades of Dry Eye.
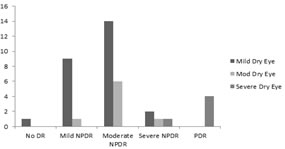
Among the No Diabetic Retinopathy group there was 1patient (25%) with Mild dry eye. Among Mild NPDR group there were 9 patients (29.03%) with Mild dry eye and 1patient (3.2%) with Moderate dry eye. Among the Moderate NPDR group there were 14 patients (53.84%) with Mild dry eye and6 patients (23%) with Moderate dry eye. Among the Severe NPDR group there were 2 patients (50%) with Mild dry eye, 1 patient (25%) with Moderate Dry eye and 1 patient (25%) with Severe Dry eye. Among the PDR group there were 4 patients (80%) with severe Dry eye.(Fig4)
Figure 4: Dry eye among different Diabetic Retinopathy Groups.
Among 70 Diabetic patients, 50 (71.43%) patients had abnormal TBUT measurements. There were 2(2.85%),14(20%),26(37.14%),4(5.71%) and 4(5.71%) patients with abnormal TBUT readings in No Diabetic Retinopathy, Mild NPDR ,Moderate NPDR, Severe NPRD and PDR groups respectively (Fig5). Figure 5: Distribution of Abnormal TBUT among the study Population.
DISCUSSION This study was aimed to derive a association of Diabetes Mellitus with Dry eye and also to correlate with severity of Diabetic Retinopathy. In our study prevalence of dry eye was 55.7% which was similar to Seifart et al.13 study with 57% of dry eye in Type I and 70% in Type II. The prevalence of dry eye was 45.6% in study done by Dhwanit Khetwani et al.14. Various other studies like Moss et al.15, Inoue et al.6, Beaver Dam eye study.16 prevalence of dry eye was18%,22.8% and 19.8% respectively. There is a large disparity in the prevalence of dry eye in various studies. This may be due to no standard set for patient selection, standardized dry eye questionnaires and objective tests. It was noted that there was higher tear film break up time abnormality (71.43%) in our study which was disproportionate when compared with Schirmer’s test. This is similar to a study in Jaipur17.This indicates unstable tear film with normal aqueous production. It may be contributed to possible abnormal function of meibomian glands in these cases. Environmental factors also play a significant role. Tear film break up time is an extremely useful test and is more informative than Schirmer’s test alone18.TBUT <2 s indicates Kerato conjunctivitis sicca(KCS)19,TBUT interval of <5 s could result in surface damage. In our study dry eye showed significant correlation with increasing grades of Diabetic Retinopathy similar to Nepp et al.20.
CONCLUSION Our study shows there is association of Diabetes Mellitus with Dry eye and there is positive correlation with severity of Diabetic retinopathy. Therefore Diabetic patients should be monitored for Dry eye signs and symptoms to prevent complications associated with it.
REFERENCES
Policy for Articles with Open Access
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.