 Home
Home
|
Table of Content - Volume 18 Issue 1 - April 2021
Santosh Y Tupdikar
Assistant Professor, Department of Ophthalmology, MIMSR Medical College, Latur, Maharashtra, INDIA. Email: skyt55@gmail.com
Abstract Background: Cataract surgery is a delicate operation fraught with complication dangers which occur intra-operatively and post –operatively and yet is the most rewarding surgery in the field of ophthalmology. Aims and Objective: To study visual prognosis of cases of scleral fixated PCIOLs and ACIOs in eyes with inadequate capsule- zonular support. Methodology: this prospective randomized interventional comparative study was conducted on 68 eyes of 68 patients in tertiary health care hospital in Mumbai, Maharashtra, from June 2014 to 2005. Result In our study we have seen that The majority of the patients were in the age group of 61-70 were 31%, followed by 51-60 were 24%; 71-80- 16%, ≤30 were 15%, 41-50 - 13%, 31-40 were 1%. The majority of the patients were Male i.e. 56.06% and Female were 43.94%. All the patients enrolled to SFIL and ACIOL equally i.e. 50%; in SFIOL 56% were Primary and 44% were Secondary where as in ACIOL 47% were primary and 53% were Secondary. Mean post operative visual Acuity Comparing SFIOL and ACIOL is statistically not –significant, but eyes secondarily implanted with IOL differ by One snellen line in Visual acuity as compared to eyes with primarily implanted IOLS. Conclusion: It can be concluded from our study that both SFIL and ACIOL cause a significant improvement in visual acuity post-operatively compared to pre-operative visual acuity. Both SFIOL and ACIOL cause significant proportion of postoperative eyes to have visual acuity ≥ 6/12. Key words: Catract, scleral fixated PCIOLs, ACIOs.
INTRODUCTION Cataract surgery is a delicate operation fraught with complication dangers which occur intra-operatively and post –operatively and yet is the most rewarding surgery in the field of ophthalmology. Rupture of posterior capsule with vitreous lost is the one of the deadest complications during extra capsular extraction of cataract. This dilemma is further complicated if surgeon want to implant a PCIOL (which is the most common mode of correction used for aphakia) which relies on posterior capsule for support. If support of anterior capsule is adequate post-capsulo rrhexis PCIOL can be supported upon it especially now that modern cataract surgery with phaco-emulsification advocates use of small anterior capsulerrhexis. PCIOL are the standard of choice in current cataract surgery. Generally, lens is placed in the capsular bag, which provides stable fixation at a position closest to the nodal point of the eye. However, there will always be instances where in the bag implantation isn’t possible, requiring that the IOL be sutured to the sclera; weakness of the lens zonules in various conditions, trauma and surgical complications during the cataract surgery are just some examples.2 Lack of capsular support is common in aphakic eyes, especially following removal of traumatic cataracts. Trans-scleral suturing of posterior chamber IOL is well-established and a good option in patients with insufficient capsular support or zonular support, either as a primary or secondary implantation. A number of reports on secondary scleral-fixated PCIOL implantation exist in the literature.1,2,3,4 However, to the best of our knowledge, primary and secondary scleral-fixated PCIOL implantation has been compared only in one study.5 Posterior capsular rupture with or without vitreous loss is the most common intraoperative complication during the cataract surgery.6,7 In the absence of adequate capsular support, the surgeon has to decide whether to perform a primary or secondary implantation. The type of anesthesia, the general medical stability of the patient and compliance, the surgical time spent to fix the complications and the surgeon's experience are factors affecting the decision-making process. In our study we have seen visual prognosis of cases of scleral fixated PCIOLs and ACIOs in eyes with inadequate capsule- zonular support
METHODOLOGY this prospective randomized interventional comparative study was conducted on 68 eyes of 68 patients in tertiary health care hospital in Mumbai, Maharashtra, from June 2014 to 2005. Intra-Ocular Lens was implanted in either primary of Secondary. The type of IOL to be inserted viz. SFIOL of ACIOL was decided on random basis however with exception that eyes of the patients compromise d comes or central degeneration shallow anterior chamber by open angles and non-constricting pupils including aniridia were selected solely for SFIOLs. Similarly, where intra capsular cataract extraction involved an intact vitreous face, ACIOL implantation was preferred so as to not disturb face all routine patients included in the study with some exclusion criteria: complicated cataract, traumatic subluxated cataracts with capsular rupture associated with corneal perforation within visual axis or angle recession or suture perforations with irregular astigmatism that may interfere with final visual result. History of closed angle or open angle glaucoma with or without previous trabeculectomy surgery done. Primary cases with nucleous fragments drop or intraocular drop which are likely to contribute to posterior segment complications. Pre-exiting retinal or macular vitreous pathology , one eyed patients . Pre-exixting corneal opacity in visual axis or where IOL implantation is combined with keratoplasty that may interfere with final visual result. Case where ACIOL or SFIOL implanted were found to have vitreous at position more than Grade ) that may it self contribute anterior segment complications . Cases where ACIOL or SFIOL implanted were found to have severe keratitis in first week due to intra operative surgical handling that may itself contribute to corneal de-compensation. All cases evaluated pre-operatively with standard ophthalmological protocols.
RESULT
Table 1: Distribution of the patients as per the Age group
The majority of the patients were in the age group of 61-70 were 31%, followed by 51-60 were 24%; 71-80- 16%, ≤30 were 15%, 41-50 - 13%, 31-40 were 1%.
Table 2: Distribution of the patients as per the sex
The majority of the patienst were Male i.e. 56.06% and Female were 43.94%
Table 3a: Distribution of the patients as per type of implantation
Table 3b: Distribution of the patients as per type of implantation
All the patients enrolled to SFIL and ACIOL equally i.e. 50% ; in SFIOL 56% were Primary and 44% were Secondary where as in ACIOL 47% were primary and 53% were Secondary.
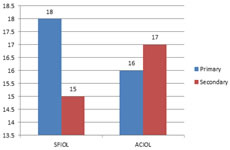
Graph 1: Distribution of the patients as per type of implantation
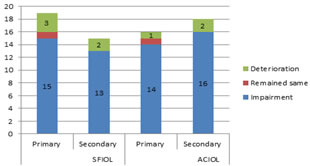
Table 4: Post-operative improvement of Visual acuity Vs Pre-operative Acuity
Graph 2: Post-operative improvement of Visual acuity Vs Pre-operative Acuity
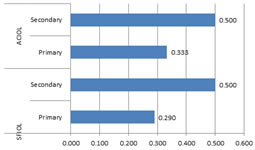
Table 5: Distribution of the patients as per the mean Visual Acuity Post-operative
Graph 3: Distribution of the patients as per the mean Visual Acuity Post-operative
Mean post operative visual Acuity Comparing SFIOL and ACIOL is statistically not–significant, but eyes secondarily implanted with IOL differ by One snellen line in Visual acuity as compared to eyes with primarily implanted IOLS.a.
DISCUSSION The endocapsular placement of an intraocular lens (IOL) is undoubtedly anatomically most preferable following successful cataract extraction. However, the presence of an unstable capsule-zonule complex or its absence, as with a dislocated lens or pseudoexfoliation syndrome, preempts the endocapsular fixation of the IOL. 9 IOL implantation in eyes that lack posterior capsular support has been accomplished in the past by using iris-fixated IOL, anterior chamber (AC) IOL and transscleral IOL fixation through the ciliary sulcus or pars plana. 9 Because of their anatomic location, scleral-fixated PC IOL's have a theoretic advantage over other IOL's with regard to complications, especially in eyes after trauma and in young patients.13,14,8 They provide better visual acuity and binocularity, lower incidence of strabismus than contact lenses, and avoid the complications of AC IOL's, which are seen more with rigid closed loop IOLs than with open-loop and irisclaw IOL's.8,11,12,10,15 In our study we have seen that The majority of the patients were in the age group of 61-70 were 31%, followed by 51-60 were 24%; 71-80- 16%, ≤30 were 15%, 41-50 - 13%, 31-40 were 1%. The majority of the patienst were Male i.e. 56.06% and Female were 43.94%. All the patients enrolled to SFIL and ACIOL equally i.e. 50%; in SFIOL 56% were Primary and 44% were Secondary where as in ACIOL 47% were primary and 53% were Secondary. Mean post operative visual Acuity Comparing SFIOL and ACIOL is statistically not –significant, but eyes secondarily implanted with IOL differ by One snellen line in Visual acuity as compared to eyes with primarily implanted IOLS.a.
CONCLUSION It can be concluded from our study that both SFIL and ACIOL cause a significant improvement in visual acuity post-operatively compared to pre-operative visual acuity. Both SFIOL and ACIOL cause significant proportion of postoperative eyes to have visual acuity ≥ 6/12 .
REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Pediatrics (Print ISSN: 2579-0897) (Online ISSN: 2636-4662) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.