 Home
Home
|
Table of Content - Volume 18 Issue 3 - June 2021
A study of clinical profile of patients with traumatic cataract
Darshana Pankaj Shah1*, Kiran Martand Bhirud2
1,2Associate Professor, Department of Ophthalmology, Dr.Ulhas Patil Medical College, Jalgaon, Maharashtra, INDIA. Email: kiranbhirud66@gmail.com
Abstract Background: Traumatic cataract is clouding of lens due to blunt or penetrating ocular trauma. Type and clinical course of cataract depends on trauma mechanism and integrity of capsular bag. Most of the traumatic cataracts are associated with ocular complications. Aim and objective: To study the clinical profile of traumatic cataract patients. Methodology: Present study was a cross sectional study carried out on patients with traumatic cataract presenting to department of Ophthalmology. Data collected was sociodemographic data, clinical history and ophthalmic examination. Data was analysed with appropriate statistical tests. Results: Most commonly affected patients were younger males. Penetrating injuries were most common and stick injury (33.33%) was most common object causing injury. Most of the patients (50%) presented to hospital within a year after injury. Total cataract 26(86.67%) was most common type of cataract observed followed by soft cataract 2(6.67%). Keywords: traumatic cataract.
INTRODUCTION Man is subjected to accidental trauma in various ways, and this may happen to any individual at any age, young people seem to be more vulnerable. Ocular trauma often leads to traumatic cataract along with damage to other ocular structures. The development of cataract is known complication following blunt or penetrating trauma to eye. In ophthalmic literature traumatic cataract accounts from 1% to 15% of all ocular injuries. In India 14% of all cases of cataract in children are due to trauma. The incidence of ocular injuries in India is estimated to be 20.5% with 75% cases occurring among those aged less than 40 years. Males are predominantly affected than females with a male to female ratio of 9:1. Cataract is the commonest complication following ocular injury.2 Combination of coup and countercoup injury along with equatorial expansion causes damage to the protoplasmic structures of the lens fibers and necrosis of the capsular material may result. The damage to the capsule impairs its semi-permeability allowing the imbibitions of aqueous by the lens substance and disturbing the active transport of metabolites associated with interstitial appearance of granules, fluid clefts and vacuoles as well as intracytoplasmic structural changes leading eventually to fragmentation and necrosis of cells and fibers, thus leading to opacification of the lens and its capsule resulting in cataract formation. 2-5 Traumatic cataract due to peforaing injury can classified as rosette cataract, localized cataract, intumescent cataract or lacerated cataract. The lenticular opacity may be vossius ring, localized or diffuse type 6-9. Cataract surgery is the important intervention for management. Traumatic cataract is most commonly observed in children and young persons. In children it may lead to loss of vision if neglected. Visual impairment in young individuals causes loss of productivity. Thus traumatic cataract has physical, social and economical impact on quality of life of younger individuals so it is important to study the clinical profile for appropriate management. Present study was conducted to see the clinical profile of patients with traumatic cataract. Aim and objective: To study the clinical profile of traumatic cataract MATERIAL AND METHODS Present study was a cross sectional study carried out in department of Ophthalmology at a tertiary health care centre. Study population was patients with traumatic cataract presenting to department of Ophthalmology. Inclusion criteria: 1. All patients with traumatic cataract of any age and both sex 2. Patients willing to participate in the study. Study was approved by ethical committee of the institute. A valid written consent was taken from the patients after explaining study to them. After considering inclusion and exclusion criteria we included 30 patients with traumatic cataract in the study. Data was collected with pre tested questionnaire. Data included sociodemographic data like age, sex, occupation etc. Detailed clinical history was noted. presenting complaints, type of injury, duration between trauma and presentation and associated ocular injury was noted. Through ophthalmic examination was done. Ophthalmic examination included Torch light examination, slit lamp biomicroscopic examination, visual acuity, indirect ophthalmoscopy, Keratometry, A-scan biometry for intraocular power calculation and B-scan ultrasonography to rule out intraocular foreign body ,vitreous haemorrhage. Data was entered in excel sheet. Data was analysed with SPSS version 23.
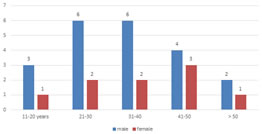
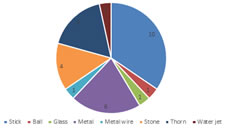
RESULTS In our study, majority of the patients were from the age group of 21-30 years (26.67%) and 21-30 years (26.67%) followed by 41-50 years (23.33%). Patients in the age group 11-20 years and 51-60 years were 13.33% and 10% respectively. (table 1) Fig 1 shows Distribution of traumatic cataract patients according to age and sex. Majority of the patients were male 21(70%) and female were 9(30%). Majority of the male patients were from the age group of 21-30 years (20%) and 31-40 years (20%). Most of the females were from 41-50 years 3(10%) and 11-20 years 3(10%). In our study, we found 73.33% patients with penetrating injuries and 26.67% patients were with 26.67%. (table 2) We studied different objects causing injury. Stick injury 10 (33.33%) was the most common object causing injury followed by metal 6(20%). Other objects causing injury were metal wire 5(16.67%), Stone 4(13.33%), glass 1(3.33%), ball 1(3.33%), thorn 1(3.33%) and wire jet 1(3.33%). (fig 2) Duration between injury and presentation to hospital is very important for management of ocular trauma. This duration varied between a week to one year. Most of the patients (50%) presented to hospital within a year after injury. 33.33% patients were presented to hospital within a month. Only 3.33% patients presented early to the hospital i.e within a week. (table 3) Total cataract 26(86.67%) was most common type of cataract observed in our study followed by soft cataract 2(6.67%). Rosette cataract and subcapsular cataract were observed in 3.33% patients each. Trauma to eye is associated with ocular damage and complications. Corneal injury 18(60%) was the most commonly seen ocular damage in our study. Iris injury was seen in 33.34% patients. Lens dislocation and vitreous harmorrhage were seen in one patient each. (table 5). In our study, associated ocular complications were Uveitis 3(10%), lens matter in anterior chamber 7(23.33%) and Glaucoma 2(6.67%).
Table 1: Distribution of traumatic cataract patients according to age group
Figure 1: Distribution of traumatic cataract patients according to age and sex Table 2: Distribution of traumatic cataract patients according to type of trauma
Figure 2: Distribution of traumatic cataract patients according to objects causing injury
Table 3: Distribution of traumatic cataract patients according to duration of trauma and presentation
Table 4: Distribution of traumatic cataract patients according to type of cataract
Table 5: Distribution of traumatic cataract patients according to associated ocular damage
Table 6: Distribution of traumatic cataract patients according to ocular complications
DISCUSSION Age wise analysis showed that majority of cases occurred in younger age group (21-40 years). This is because of the greater involvement in outdoor activity and recreational activity and work pattern of people. Most injuries resulted from stick followed by metal. Other studies also showed an increased incidence of traumatic cataract in younger age group. Daljit Singh showed similar age group distribution.10 This study showed a male preponderance (72.5 %). This is because men are more exposed to ocular trauma because of occupation and they are from age earning group. We studied different objects causing injury. Stick injury 10 (33.33%) was the most common object causing injury followed by metal 6(20%). Other objects causing injury were metal wire 5(16.67%), Stone 4(13.33%), glass 1(3.33%), ball 1(3.33%), thorn 1(3.33%) and wire jet 1(3.33%). Krishnamachary M also found that most of the injuries i.e., 54.7% were caused by stick or bow and arrow.11 Penetrating trauma was found in more numbers of cases, because most of the patients were manual laborers from rural areas. The penetrating injury usually leaves a scar on the cornea. The visual prognosis in traumatic cataract is poor because of concomitant injury to other structures. The management of traumatic cataract depends on integrity of posterior capsule, zonular apparatus and associated injury to cornea, uveal tissue and posterior segment. In this study the associated damages were corneal injuries in the form of scar or opacity seen in 18 cases (60%), corneal scarring and opacity affected the visual acuity by obstructing the visuals axis and causing astigmatism. Injury to the iris was seen in 13 cases (33.34 %) in the form of traumatic mydriasis, iris prolapsed through corneal tear, iridodialysis and adherent leucoma. Similar to our study, Marcus Blum et al. 12observed corneal injury (61.9%), iris related injury (52.3%) and dislocated lens (35.2%). Krishnamachary et al. 11showed corneal injury in 60% patients, iris injury in 49.6% patients and dislocated lens in 3% patients. In a study by Daljit singh, 37% patients had corneal injury.10 In our study, associated ocular complications were Uveitis 3(10%), lens matter in anterior chamber 7(23.33%) and Glaucoma 2(6.67%). Similar to our study, Marcus Blum noted Lens matter in anterior chamber associated with uveties15 in 4% of cases.
CONCLUSION Penetrating injuries mainly lead to traumatic cataract. Total cataract is commonest form of traumatic cataract. Various ocular injuries and ocular complications are associated with traumatic cataract.
REFERENCES
Policy for Articles with Open Access
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.