 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 10 Issue 2 - May 2019
Influence of accelerated cast change interval in the Ponseti method: Study from rural and semi urban
B Sreekanth Rao1, Cheeti Srinivas Kalyan Rao2*, G V S Moorthy3
{1Assistant Professor, 3Professor, Department of Orthopaedics}{2Associate Professor, Department of Paediatrics} Bhaskar Medical College and Bhaskar General Hospital, Yenkapally, Telangana, INDIA. Email:skrao78@gmail.com
Abstract Background:Ponseti method has proved to be an excellent outcome in the management of club foot. Ponseti method is a reliable and efficient way to manage club foot deformity when treatment is started early. Aims and Objectives: To evaluate the influence of the accelerated cast change interval on treatment outcomes by the Ponseti method. This case series is to spread awareness by showing the results of this technique used in semi urban centre. Materials and Methods: The case study was conducted at Bhaskar General Hospital, Yenkapally, Telangana from August 2017 to December 2018 and was followed up till April 2019. All the club feet patients reported to either Paediatric or Orthopaedic Outpatient and were taken for the study and the patients between birth and 12 months of age of either sex, were screened by Paediatrician for any associated problems and syndromes and only Idiopathic club feet were selected for the study. The selected 24 infants were treated between 07 days to 5months of age, out of which, 16 were male and 08 were female. Five male and one female infant had bilateral CTEV accounting to total of 30 feet. The majority of participants, nineteen infants (80%) were from rural Moinabad and five (20%) were from around semi urban Moinabad. General hygiene and maintenance was poor, which required frequent cast changes necessary in rural population. These cases were thus taken up for accelerated cast change study of Ponseti method. In the present case series, 24 cases of idiopathic clubfoot were treated by Ponseti method and assessed by Pirani scoring system. Cast was changed at an interval of 03 days for 4 to 5 weeks. The number of casts applied was, 09 to 11. Tendo Achilles tenotomy was done if required. The patients were followed upto one year of age from the removal of their last cast. Results: Correction was achieved in all the patients. Tendo Achilles tenotomy was performed in 83.3% of the patients. The Pirani score improvement was observed in all the 24 cases.Conclusion: Accelerated cast changes following the Ponseti technique did give good results as it was practised under supervision of well trained faculty and staff. It is good to spread the message of accelerated version of Ponseti method, that it can safely be used in the treatment of club foot correction. Keywords: Ponseti method, Accelerated cast, Idiopathic club foot, Tenotomy.
INTRODUCTION Clubfoot is regarded as a developmental anomaly. A normally developing foot turns into a clubfoot during the second trimester of pregnancy. Ponseti described the clubfoot deformity as occurring mostly in the tarsus1.It has been identified in the mummified remains of the Egyptian body of King Tutankhamen as well as in several other individuals in history as well as in contemporary times2. The Ponseti Method has become the gold standard of treatment compared to the other interventions because of its better outcomes 3. It is widely used for the management of clubfoot. It consists of two distinct phases, the correction phase and the maintenance phase. The correction phase involves precise manipulation of the foot around the talus to correct the cavus, adductus and varus of the deformity. The standard Ponseti method uses weekly foot and leg plaster changes to gradually correct the deformity, using a strictly defined sequence of moulded plaster changes. A percutaneous tenotomy of the Achilles tendon is usually performed to correct the residual equinus. The maintenance phase involves the use of a foot abduction brace for 23 hours a day for three months, followed by nightly use until four to five years of age4 . Percutaneous Tendo Achilles tenotomy and later tibialis anterior transfer may be used but are not always necessary5. The Pirani score6 and the Dimeglio score7 are two of the most widely used classification systems for clubfoot deformity8. The Pirani score is from 0 to 6 where zero is a normal foot and six is the most severe deformity. It is reliable when used by non-specialist health workers9. The Dimeglio score has a maximum of 20 points and the deformity is graded as benign, moderate, severe or very severe. We hypothesized that a three-day interval might be as effective as weekly plaster changes.
MATERIALS AND METHODS In the present case series, 24 cases of idiopathic clubfoot were treated by Ponseti method and assessed by Pirani scoring system. This study was conducted at Bhaskar General Hospital, Yenkapally, Telangana from August 2017 to December 2018 and followed-up till April 2019. Ethical approval was obtained from the Bhaskar medical college Ethics Committee. All the club feet patients reported to either Paediatric or Orthopaedic Outpatient and were taken for the study and the patients between birth and 12 months of age of either sex, were screened by Paediatrician for any associated problems and syndromes and only Idiopathic club feet were selected for the study.The selected 24 infants were treated between 07 days to 5months of age, out of which, 16 were male and 08 were female. Five male and one female infant had bilateral CTEV accounting to total of 30 feet. The majority of participants, nineteen infants (80%) were from rural Moinabad and five (20%) were from around semi urban Moinabad. General hygiene and maintenance was poor, which required frequent cast changes necessary in rural population. These cases were thus taken up for accelerated cast change study of Ponseti method. In the present case series, 24 cases of idiopathic clubfoot were treated by Ponseti method and assessed by Pirani scoring system. Cast was changed at an interval of 03 days for 4 to 5 weeks. The number of casts applied was, 09 to 11. Tendo Achilles tenotomy was done if required. The patients were followed upto one year of age from the removal of their last cast. Using a prescribed format, the data was collected, assessed, analysed and compared with other series and observations were made. 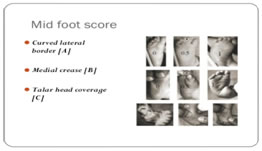
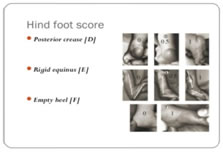
Figure 1: PIRANI MID FOOT SCORE Figure 2: PIRANI HIND FOOT SCORE CASE: 1
Figure 3: CTEV right foot Figure 4: Third week Ponseticorrection
Figure 5:Fourth week ponseti correction and ponseti shoes with bar
CASE 2 Figure 6:First and second week left foot Ponseti correction Figure 7:Ponseti cast figure 8 ponseti shoes with bar
RESULTS The study shows that the correction was achieved in all the patients. Tendo Achilles tenotomy was performed in 80.3% of the patients. Cast was changed at interval of 03 days for 5 weeks. The Pirani score improvement was observed in all the 24 cases.
DISCUSSION Ponseti method has become the standard method of treating children with clubfoot deformities10,11.Our results suggests that good results can be achieved with an accelerated method, changing the plaster in 5 days per week. According to Giesberts RB et al12, a study was performed by systematically reviewing the existing literature, dealing with the Ponseti method regarding the influence of cast change interval on treatment outcomes. All feet were scored using the Pirani method13, and comparative studies in which the cast change interval was varied, scientific databases were searched for relevant publications. Synthesis tool was used in their study to evaluate the results of the studies and derive conclusions from relevant clinical outcomes. The outcome of this study is similar to the results of this study. The authors Morcuendeet al found that an accelerated five-day interval can be equally effective14 ,they were concerned that further acceleration in the casting might give rise to problems like swelling in the cast,14 No patients developed this problem in our study and the results were similar to this study. Harnettet al15 further accelerated the regimen to three times a week and got comparable results. They did not come across any problems which Morcundeet al14 had suggested with faster regimens. The results of their study are similar to the present study. There are well proven factors that have contributed towards the research in decreasing interval between cast applications as part of the Ponseti clubfoot correction. Firstly, there is evidence to favor that shortening cast time for the idiopathic congenital clubfoot deformity gives objective good results.14-16,17Secondly, there are lot of problems, inconvenience to the patients and their family, who travel long distances over a period of eight to twelve weeks, from distant places to clinics for treatment. The time away from home, loss of working hours, economic burden on family all of which are a common concern in developing countries, may be greatly improved if the duration of treatment is cut short14,18. This could provide great savings for costs incurred while staying away from home and time lost from work. In turn, compliance may also benefit. The patients who come from remote areas can be counselled and convince them to be admitted for this period and upon application of the last cast after tenotomy can be discharged with a foot abduction brace. This could reduce hospital stay to three weeks. General hygiene and maintenance was poor required frequent cast changes in rural population. This promoted to change cast early and this study was achieved. They can be instructed to remove the cast after three weeks and continue the treatment with braces thereafter. Thirdly, less time of immobilization in plaster is quite advantageous for the baby in view of reduced skin sore issues, easier bathing, more normal motor development and possibly lessens the risk of osteopenia19. It is important to appreciate that all accelerated casting studies and trials have addressed the idiopathic congenital clubfoot, and that the effects and use in syndromic 20 or complex clubfoot types 21 are unknown. Some of the limitations of this study include the relatively small sample size, and the short period for data collection. The study also did not have a long follow up to show whether there is more recurrence in the accelerated Ponseti group or not.
SUMMARY A prospective study was done with the aim to evaluate the influence of the accelerated cast change interval on treatment outcomes by the Ponseti method and to spread awareness by showing the results of this technique used in semi urban centre. The selected 24 infants were treated between 07 days to 5months of age. The selected 24 cases of idiopathic clubfoot were treated by Ponseti method and assessed by Pirani scoring system. Cast was changed at an interval of 03 days for 4 to 5 weeks. The number of casts applied was, 09 to 11. Tendo Achilles tenotomy was done if required. The patients were followed upto one year of age from the removal of their last cast. The study shows that the correction was achieved in all the patients. Tendo Achilles tenotomy was performed in 83.3% of the patients. The Pirani score improvement was observed in all the 24 cases.
CONCLUSION Accelerated cast changes following the Ponseti technique did give good results as it was practised under supervision of well trained faculty and staff. Correction was well achieved in shorter duration. Recurrence is not observed till date in the follow-up. It is good to spread the message of accelerated version of Ponseti method, that it can safely be used in the treatment of club foot correction. A larger study and more research are required to determine the optimal cast change interval and to evaluate the long-term effects of shorter cast change intervals.
REFERENCES
|
|




 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.