 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 11 Issue 2 - August 2019
Functional outcome of arthroscopy assisted anterior cruciate ligament reconstruction using quadrupled hamstring autograft
Shashikant B Kukale1, Aniket A Hajare2*
1Associate Professor, 2Junior Resident-3, Department of Orthopaedics, Government Medical College and Hospital, Latur. Near old railway station, Mataji Nagar, Moti Nagar, Latur, Maharashtra. Pin- 413512, INDIA. Email: aniketahajare89@gmail.com
Abstract Background: The knee joint is the most complex and commonly injured of all joints and the anterior cruciate ligament is the most commonly injured ligament. Recent studies showed an improvement in the outcome of ACL reconstruction using semitendinosus and gracilis tendons. Aim: To evaluate the functional outcome of arthroscopy assisted anterior cruciate ligament reconstruction using quadrupled hamstring autograft. Material and Methods: A total of 30 patients both male and female having traumatic anterior cruciate ligament tear with or without associated lesions that were identified radiologically or arthroscopically were included. They were treated by arthroscopically assisted anterior cruciate ligament reconstruction using quadrupled hamstring autograft. Patients were followed up for 6 months postoperatively. Results: Of the 30 patients assessed, 27 patients achieved full range of motion postoperatively within 4-6 weeks. But 3 patients had flexion ranging up to 90 till 6 weeks postoperatively. As per the Lysholm scoring system, 27 patients (90%) had an Excellent outcome; 3 (10%) had a Good (72-90) outcome and as per 2000 IKDC scoring system, 21 patients (70%) had ‘Normal’ outcome; 9 (30%) had ‘Nearly Normal’ outcome. Conclusion: Arthroscopic ACL reconstruction with the quadrupled hamstring tendon provides excellent subjective and functional results in the patients and the procedure has little morbidity, low reoperation rate, and excellent clinical results. Key Word: Arthroscopy, Anterior cruciate ligament reconstruction, quadrupled hamstring autograft, functional outcome
INTRODUCTION The Anterior Cruciate Ligament (ACL) is regarded as critical to the normal functioning of the knee. Today’s modern world of high speed motorbikes and active athletic sports has led to increased ligament injuries of the knee. The knee joint is the most complex and commonly injured of all joints and the anterior cruciate ligament is the most commonly injured ligament.1The anterior cruciate ligament forms the pivot in the functional congruence and stability of the knee in association with the other ligaments, capsule, muscles, and bone.2,3 Over the period of past couple of decades, the knowledge of ACL regarding its anatomy, biomechanics, epidemiology, graft sources, fixation methods and clinical outcomes of ACL reconstruction, has increased manifold. ACL reconstruction can now be done consistently and predictably. Successful reconstruction of the Anterior Cruciate Ligament has been described by numerous authors worldwide using different types of donor autografts viz. tendons of patella, hamstring or quadriceps and allografts. Recent studies showed an improvement in the outcome of ACL reconstruction using semitendinosus and gracilis tendons.4-6 With the semitendinosis, using the multiple bundle technique and improved fixation with the endo-button, has made the graft stronger and stiffer. The endo-button made the procedure endoscopic, and eliminated the need for the second incision. Use of biodegradable interference screw to fix the graft at the tunnel entrance produces a graft construct that is strong, short, and stiff. This study was conducted to evaluate the functional outcome of arthroscopy assisted anterior cruciate ligament reconstruction using quadrupled hamstring autograft.
MATERIAL AND METHODS Study design:Prospective and retrospective study including 30 patients who underwent arthroscopically assisted anterior cruciate ligament reconstruction using quadrupled hamstring autograft over a period of two years. Patients both male and female having traumatic anterior cruciate ligament tear with or without associated lesions that were identified radiologically or arthroscopically were included. The diagnosis was made on the basis of combination of symptoms, signs and radiological and arthroscopic findings. Inclusion criteria
Exclusion criteria
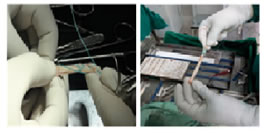
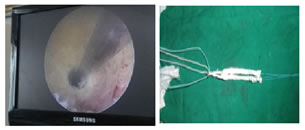
Preoperative assessment: On visit of patient to OPD or casualty department, detailed history was taken with regard to nature of injury, duration since injury, mechanism of injury, symptoms, associated injury, details of primary treatment taken and past medical illness. Detailed general and systemic examination was carried out. Assessment of injured knee status was done. Special tests for knee assessment including lachman test, anterior drawer test, pivot shift test, varus/valgus test, Mcmurray`s test, posterior drawer test were carried out to reach at a provisional diagnosis. Thus, having arrived at a provisional diagnosis of ACL tear, further investigations were carried out. These investigations included MRI of involved knee to confirm diagnosis and to rule out associated lesion. Radiograph of involved knee-anteroposterior, lateral views for segond’s fracture (i.e. chip fracture of lateral condyle of tibia indicating ACL tear). In acute cases of ACL injury, patients were treated conservatively with cylindrical slab or long knee brace for about 3 weeks following which ACL reconstruction was planned, once patient achieved adequate hamstring and quadriceps function. In this study MRI confirmation of ACL injury was done in all patients with diagnostic arthroscopy and ACL reconstruction was carried out at the same time. Associated injuries were treated at the same time as ACL reconstruction. Procedure: Choice of anaesthesia was decided by anaesthetists and the same informed to patient. Most of the cases were done under spinal anaesthesia. Firstly, anterolateral and anteromedial portals were made for standard arthroscopy and knee examined for ACL tear. Once ACL tear was confirmed arthroscopically, the procedure was carried forward. The associated injuries like meniscal injuries were treated by either suturing or partial meniscectomy. Procedure was done in following steps such as graft harvesting, graft preparation, notch preparation, tibial and femoral tunnel placement, Graft passage and fixation and closure Figure 1: Graft harvesting Figure 2: Graft preparation Figure 3: Arthroscopic Tibial and Femoral tunnel preparation; Figure 4: Endobutton with graft
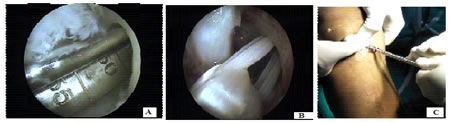
Figure 5: A. Measurement of Femoral tunnel; B. Passage of graft and Endobutton through femoral tunnel C. Graft fixation with Interference screw
During the rehabilitation process, the patient has been observed closely, initially at every 1-2 weeks and later at every 4-6 weeks intervals, as per the protocol. Figure 6: Active knee flexion; Figure 7: Full weight bearing with walker RESULTS We had 14 patients (47%) in the age group 15-25 years, 10 patients (33%) in the age group 26-35 years and 6 patients (20%) in the age group 36-45 years. There were 28 male patients (93%) and 2 female patients (7%). In our study, isolated ACL tear was present in thirteen patients (43%). In 10 patients (33%), ACL tear was associated with medial meniscus tear; in 3patients (10%), with lateral meniscus tear; and in 4 patients (14%), with both medial and lateral meniscus tear. Fourteen patients (47%) had right sided anterior cruciate ligament tear and sixteen patients (53%) had left sided anterior cruciate ligament tear. Table 1: Distribution of pathological lesions in study group
The mode of injury was Road Traffic Accident (RTA) in seven patients (23%), most commonly involving two wheeler drivers. Nine patients (30%) had injury during sports activities like kabaddi, football, badminton. Fourteen patients (47%) had injury because of fall due to twisting injury. Five patients who presented to us within first 6 weeks of ACL tear, had no associated meniscal lesions. Out of 8 patients who presented to us within 6 weeks to 3 months duration of ACL tear, 3 patients (37.5%) had developed associated meniscal lesions. Out of 6 patients who presented to us within 3 months to 6 months duration of ACL tear, 3 patients (50%) had developed associated meniscal lesions. Out of 6 patients who presented to us within 6 months to one year duration of ACL tear, 4 patients (67%) had developed associated meniscal lesions. All 5 patients (100%), who presented to us after 1 year of ACL tear, had developed associated meniscal lesions.
Table 2: Association of meniscal lesions with duration of 1stpresentation
In our study, as per the Lysholm scoring system, 27 patients (90%) had an Excellent outcome; 3 (10%) had a Good (72-90) outcome; no patient had Fair or Poor outcome.
Table 3: Grading of results as per Lysholm score
In our study, as per 2000 IKDC scoring system, 21 patients (70%) had ‘Normal’ outcome; 9 (30%) had ‘Nearly Normal’ outcome; no patient had ‘Abnormal’ or ‘Severely Abnormal’ outcome. Table 4: Grading of results as per 2000 IKDC score
DISCUSSION The anterior cruciate ligament serves an important stabilizing and biomechanical function for the knee. Reconstruction of the ACL remains one of the most commonly performed procedures in the field of sports medicine. The theoretical advantage of arthroscopic surgery includes less injury to patellofemoral mechanism and possibly less frequent symptoms and contractures of the patellofemoral joint post-operatively. The proper site for location of bone tunnels can be better identified by an arthroscope. At present the most commonly used grafts for ACL reconstructions are bone-patellar tendon-bone autograft and hamstring tendon autografts. Kang et al7prospectively reviewed 21 patients after ACL reconstruction with quadrupled semitendinosus tendon and Endobutton at one-year post-operative period. The outcomes showed improved knee functions. Biau et al8 concluded that morbidity was lower for hamstring autografts than for patellar tendon autografts. In our study, we used semitendinosus graft in 27 patients and combined semitendinosus and gracilis graft in 3 patients. This technique using quadrupled semitendinosus reconstruction had little morbidity, low reoperation rate, and excellent clinical results. Pinczewski et al9studied the use of intra-operative landmarks and found that it resulted in reproducible placement of the tunnels and an excellent clinical outcome seven years after operation. Vertical inclination was associated with increased rotational instability and degenerative radiological changes, while rupture of the graft was associated with posterior placement of the tibial tunnel. If the osseous tunnels are correctly placed, single-bundle reconstruction of the ACL adequately controls both anteroposterior and rotational instability. In our studies all the patients with excellent and good outcomes had posteriorly angled tibial tunnel in sagittal plane. In the lateral view all the patients had tibial tunnel placement at55° with joint surface. Howell et al10 stated that in arthroscopic anterior cruciate ligament reconstruction, tibial tunnel position dictates the femoral tunnel position to a large extent. He added that ideally tibial tunnel must be angled in medial to lateral direction and in sagittal plane it should be angled posteriorly. It has been popular to place the femoral tunnel at the so called 11’0 clock position to replicate the origin of anteromedial bundle of ACL. Loh et al11 published that the 10’0 clock position more effectively resists rotatory loads when compared to 11'0 clock position. Scoop12published that the best position for the femoral tunnel is between 10 and 11’0 clock in the right knee and between 1 and 2’0 clock in the left knee. In this series of the 30 patients with excellent and good outcome, all patients had the femoral tunnel in antero-posterior view within the 10’O clock to 11’O clock for the right knee and within 1’O clock to 2’O clock in the left knee. We detected no significant difference in the outcomes, as measured by lysholm knee score and IKDC score, related to whether the left or the right knee was involved, the patient’s age, sex, whether the instability occurred following a road traffic accident, fall or sporting injury. In our study it was found that meniscal injuries increase with the duration of the torn ACL. Patients with concomitant meniscal injuries had more pain and lower lysholm score after arthroscopic anterior cruciate ligament reconstruction compared to those with intact menisci. ACL reconstruction procedure is efficient in restoring a satisfactory stability for patients and stabilises evolution of degenerative lesions. We used Lysholm scoring system and 2000 IKDC scoring system for subjective evaluation of patients at their follow up. Buchner Met al13in their clinical study evaluated clinical, functional, radiological and isometric results after arthroscopic reconstruction of ACL. Seventy operated patients with an average age of 34.3 years could be clinically examined at a mean follow-up time of 6 years. The preoperative activity level could be maintained in 71% of the patients. The Lysholm score showed ‘excellent’ and ‘good’ results in total 85% patients; with a mean score of 83.6%.As of Lysholm and Gilquist Knee Scoring, we compared our results to the results of Lysholm and Gilquist.14 They had studied 60 cases totally and had excellent and good results in 88%. They had 8 % with fair results and 4% poor outcomes.In our study, average Lysholm score was 95.76 at mean follow up period of 12 months. The Lysholm score showed ‘excellent’ results in 27 patients (90%) and ‘good’ results in 3 patients (10%). No patient had either ‘fair’ or ‘poor’ result. Anderson et al15compared six knee ligament rating scales in a study of seventy patients and concluded that the International Knee Documentation Committee (IKDC) scale should be used as the standardized measurements. Daniel O'NeiI16had evaluated 45 patients of arthroscopic ACL reconstruction with IKDC scoring. In his study, 92% patients had ‘normal’ or ‘nearly normal’ outcome and 8% had ‘abnormal’ outcomes. Cooley VJ et al182 in their study on 20 ACL reconstructions and stated that activity level was maintained at the preinjury level in nearly half the patients. Isokinetic strength deficits were less than 10%; 17 (85%) of the patients had a normal or nearly normal result as graded by the IKDC scoring system. In our study, as per 2000 IKDC scoring system, 21 patients (70%) had ‘Normal’ outcome; 9 (30%) had ‘Nearly Normal’ outcome; no patient had ‘Abnormal’ or ‘Severely Abnormal’ outcome. Chen L et al17 in their study used quadrupled semitendinosus auto graft for ACL reconstruction using the endobutton for femoral fixation and later they used this technique for over 10 years with no known instance of fixation failure at the femur or tibia. In this study, we used endobutton for femoral fixation and metal interference screw for tibial fixation of graft. Using these implants we achieved stable graft fixation without any instance of fixation failure. In our study, of the 30 patients assessed, 27 patients achieved full range of motion postoperatively within 4-6 weeks. But 3 patients had flexion ranging up to 90° till 6 weeks postoperatively, as they did not follow proper rehabilitation program in the early postoperative period. After giving them graduated supervised physiotherapy for hamstring and quadriceps strengthening, range of motion improved in all 3 patients. In our study, 2 patients had 1+ laxity on anterior drawer test. These patients had no instability while walking, running, climbing down stair. All other patients had negative anterior drawer and lachman test. Pivot shift test was negative in all patients. All patients managed to achieve significant one leg hop distance as compared with unaffected side after 6-8 months postoperatively. Manjappa and Srinivas18 in their study of 20 patients, found that most of the study subjects had regained hamstring strength by 3rd post-op month. There were no other morbidities reported during the follow-up. In our study although there was decreased hamstring strength initially, there was not much difference in the strength of hamstrings at final follow up. All patients in our study returned to pre injury level of activity and sports after 6-8 months postoperatively.None of the patients in our study had major complication following surgery.
CONCLUSION Arthroscopic ACL reconstruction with the quadrupled hamstring tendon provides excellent subjective and functional results in the patients and the procedure has little morbidity, low reoperation rate, and excellent clinical results.
REFERENCES
|
|


 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.