 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 12 Issue 2 - November 2019
Nandkishor Goyal1*, Prashant More2, Bhavatu Patel3, Avanish Rai4
1,2,3,4Department of Orthopaedics, ACPM Medical college, Dhule, Maharashtra, INDIA. Email: nandkishor596@gmail.com
Abstract Background: The tension band wiring technique a common treatment for the fixation of olecranon fracture with three fragments. Fracture of olecranon process of ulna are considered among the few most commonly encountered fractures in emergency room (approximately 10% fractures around adult elbow). Surgical management for these fractures include various options most commonly used is tension band wire reconstruction which converts tensile distraction force of triceps into dynamic compressive force across the olecranon articular surface. Methods: We reviewed 10 patients (6female and 4 male) with median age group 45yrs (range: 30-60yrs) who underwent TBW osteosynthesis for isolated olecranon fractures. Time between the trauma and surgery is average 3 days. In one patient we had compound and communicated fracture in whom time lapse was 10 days. All patients were assessed clinically by measuring flexion-extension and pronation-supination arcs as well as radiologically with elbow X-Rays. Surgery was performed after physician and anesthesia fitness under intravenous regional anesthesia. We had inserted 2 Kirschner wires from the tip of olecranon across the fracture into to distal fracture fragment of ulna. Further we passed the cerclage wire around the Kirschner wires in the figure of 8 pattern and through the hole in distal ulna. Then slab in 110o of flexion was applied. Stitches were removed after 15 days and then cast was applied for eight weeks and after clinical and radiological review, we started physiotherapy. Conclusion: Tension band wire fixation has been considered gold standard in fixation of fracture of olecranon process of the ulna. Key Word: olecranon fracture, tension band wiring.
INTRODUCTION Fractures of the olecranon account for up to 40 % of all fractures around the elbow joint. An uncomplicated fracture of the olecranon is considered to be a common injury. The main goal of tension band wiring (TBW) is the exact repositioning of the articular surface and the re-establishment of stability in the humero-ulnar joint. The olecranon process of the ulna articulates with the trochlea of the humerus. This articulation forms the true hinge type of joint allowing movement only in one plane. The obliquity at ulnohumeral articulation is also responsible for formation of carrying angle (angle formed by long axis of humerus as the long axis of the ulna projects on the plane containing the humerus or angle formed by the long axis of the ulna and the projection of the long axis of the humerus onto the plane of the ulna). The olecranon process of the ulna has important function to prevent anterior subluxation of ulna. Proximal ulna fractures constitute about 10% of fractures around elbow. This study aims to look for the outcome treatment and results of tension band fixation of commonly encountered fracture of olecranon process of the ulna. Therefore, we examined pre-, intra- and postoperative radiographs for fracture classification and imperfections in the TBW in order to prove that the technique should be used more precisely.
MATERIAL AND METHODS Inclusion criteria
Exclusion criteria
OBSERVATION We examined 10 patients out of which 6 were females and 4 were males with median age group 45yrs ranging from 30yrs to 60yrs who underwent TBW osteosynthesis for isolated olecranon fractures. Time lapse between the day of trauma and day of surgery was on an average of 3 days; except in one patient who had compound and communitated fracture so we had to wait for complete healing of the wound and complete the course of intravenous antibiotic inections. All patients were assessed clinically by measuring flexion-extension and pronation-supination arcs as well as radiologically with elbow X-Rays. Patients were grouped depending on Mayo classification types as it is one of the most acceptable classification. Surgery was performed strictly after complete routine blood and urine check up followed by physician fitness and then pre-anesthetic check up. Most commonly surgeries were performed under intravenous regional anesthesia. We had inserted 2 kirschner wires from the tip of olecranon across the fracture into to distal fracture fragment of ulna. Further we passed the circlage wire around the kirschner wires in the figure of 8 pattern and through the hole in distal ulna. Then slab in 110o of flexion was applied. Stitches were removed after 15 days and then cast was applied for six weeks and after clinical and radiological review, we started physiotherapy.
RESULT Our study included six females and four males with a mean age of 45(30-60). Four were Mayo type II-A and three were Mayo type II-B two were Mayo type III-A and one of Mayo type III-B. Eight patients had no complications post-operatively with good outcome, full rotational ROM and mean flexion arc of 20-170°. One patient had range of motion between 40-90° with full rotational ROM. No non-unions were noted in our series. Our results are better than what given in reference. All patients except one had very good to excellent results. Table 1: Table showing Patients details
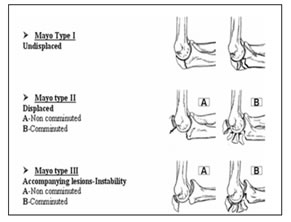
Figure 1: figure showing the Mayo classification for the olecranon fractures which is based on displacement of fracture, subluxation of articulation, and presence of communition Figure 2: 38yrs/ female Compound fracture Mayo type III-B Pre-op x-ray; Figure 3: 38yrs/ female compound fracture Mayo type iii-b immediate post-op x-ray; Figure 4: 42yrs/ female Closed fracture Mayo type II-A Pre-op x-ray; Figure 5: 42yrs/ female Closed fracture Mayo type II-A Immediate Post-op x-ray
DISCUSSION The literature and surgeons refer to TBW as a simple, cost-efficient and easily performed procedure. Majority of proximal ulna fractures are treated surgically. Simple olecranon fractures can be reconstructed by various methods which include tension band wiring, plating, and intramedullary rod; tension band wiring being gold standard. Tension band wiring is selectively suitable here as the triceps (an extensor muscle) play role of major deforming force causing the bending moment at discontinuity. After achieving accurate reduction, stainless steel band wire is applied in figure of 8 pattern around two parallel Kirschner wires (prevent slippage of band wire on tension surface of bone and joint movements). These parallel kirschner wires act as rails along which bone fragments can slide during dynamic compression exerted in active flexion. As triceps moves proximal fragment, the tension band wire, which is on outermost surface of olecranon, keeps two fragments together and maintains the point of contact. Tension band exerts the reactive compressive forces across the fracture surfaces. This is balanced by equal and opposite tensile force in wire. Because of rural and uneducated population, patients are likely to disobey instructions given by doctors; so we gave post-op immobilization for six weeks. Mechanism of injury: Subcutaneous position of the olecranon on posterior aspect of elbow makes it more vulnerable for injury. Fractures of the olecranon process of the ulna are typically due to direct blow to the olecranon process. Among indirect mechanisms, most common injury is fall on outstretched hand with semiflexed elbow and supinated forearm in which the triceps snaps the olecranon over lower end of the humerus which acts as fulcrum. Olecranon fracture is a type of avulsion fracture due to pull of triceps muscle. Conclusion and message: Parallel kirschner wires act as rails along which bone fragments can slide during dynamic compression exerted in active flexion. As triceps moves proximal fragment, the tension band wire, which is on outermost surface of olecranon, keeps two fragments together and maintains the point of contact. So tension band wiring is considered as gold standard for fixation of olecranon fractures of the ulna.
REFERENCES
|
|

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.