 Home
Home
|
Table of Content - Volume 14 Issue 2 - May 2020
Functional outcome of antegrade intramedullary interlocking nailing in fracture shaft of humerus
A T Senthil Kumar1, Vivekanandhan2*
1Associate Professor, 2Senior Resident, Department of Orthopaedics, Melmaruvathur Adhiparasakthi Institute of Medical College Science Hospital And Research Institute, GST Road, Melmaruvathur, Tamilnadu, INDIA. Email: drvenkatesh19@gmail.com
Abstract Background: The aim is to prospectively study the “Functional outcome of Antegrade Intramedullary Interlocking nailing in fracture shaft of humerus. Materials and Method: This prospective study was conducted at Department of orthopaedics, Melmaruvathur Adhiparasakthi Institute of Medical science, Melmaruvathur. who attended in OPD. Our study is a case series of 20 diaphyseal fractures in 20 persons treated with Antegrade Intramedullary Interlocking nailing. Results: A series of 20 cases of fracture shaft of humerus treated by antegrade intramedullary interlocking nailing were studied. The results of the use of intramedullary nailing for the diaphyseal fractures of the humerus have been mixed, with some studies showing good outcome and some others poor outcome. Conclusion: Locked intramedullary nailing is a novel treatment option for diaphyseal fractures of the humerus. It is ideal in treating diaphyseal fractures of the humerus in patients when other treatment methods are likely to fail, like those with osteoporosis, severely comminuted segmental fractures and polytrauma where reduction in operating time and early rehabilitation are the primary objective. Nail length should be chosen carefully and it may be errored on the shorter side rather than the longer side. Do not distract the fracture site by trying to impact a nail that is excessively long. Locked intramedullary-nailing is an effective and safe alternative for the treatment of diaphyseal humeral fractures. It is suitable for treatment in patients with osteoporosis, pathological fractures, polytrauma and associated neurovascular injuries. It helps in providing early rehabilitation and lessens the morbidity. Key Words: Antegrade intramedullary interlocking, nailing, fracture, trauma.
INTRODUCTION Fractures of the humeral shaft are relatively common injuries. The uniqueness in the anatomy, the fracture configuration and the functional significance of the region influences the treatment options. Humeral shaft fractures account for approximately 3% of all fractures3. Nonsurgical management of humeral shaft fractures with functional bracing gained popularity in the 1970s, and this method is arguably the standard of care for these fractures. Still, surgical management is indicated in certain situations, including polytraumatic injuries, open fractures, vascular injury, ipsilateral articular fractures, floating elbow injuries, and fractures that fail nonsurgical management. Surgical options include external fixation, open reduction and internal fixation, minimally invasive percutaneous osteosynthesis, and antegrade or retrograde intramedullary nailing. Each of these techniques has advantages and disadvantages, and the rate of fracture union may vary based on the technique used. A relatively high incidence of radial nerve injury has been associated with surgical management of humeral shaft fractures7. However, good surgical outcomes can be achieved with proper patient selection. The sleeve of muscles surrounding the bone and the rich vascularity provided by them helps in fracture healing. The mobility of the shoulder and the elbow joint accommodates for a minimal degree of angulation and shortening. Moreover the limb does not take part in weight bearing or ambulation; hence some amount of shortening is functionally acceptable. Because of all these inherent advantages of the region, conservative treatment results in very gratifying outcome23. Treatment of humeral diaphyseal fractures has centred on nonoperative techniques, which have been providing excellent functional results. The main disadvantage of shoulder stiffness has been overcome by the functional bracing techniques. Although most of these fractures can be treated nonoperatively, indications for operative intervention have been well reported. Ultimately, optimal results depend on matching the treatment alternative with the character of the fracture and the needs of the patient. Open reduction and internal fixation with plate osteosynthesis supplemented with bone grafting has been the gold standard for treatment of fractures of the humeral diaphysis32. Though plate fixation has given high rates of union, it involves extensive soft tissue stripping,potential injury to radial nerve and poor fixation in osteoporotic bone. Intramedullary fixation devices have been introduced as they have been used very effectively in the treatment of lower limb fractures. Interlocking intramedullary nailing is being evaluated for its effectiveness in the treatment of humeral diaphyseal fractures. The advantages of intramedullary nailing are minimal surgical exposure, better biological fixation, and minimal disturbances of soft tissues and early mobilization of neighbouring joints17. The technique of interlocking nailing represents the newer approach of the treatment of humeral fractures. Interlocking nailing also avoids complications like lack of rotational control, migration of nail and requirement of supplementary bracing. Hence the method of Antegrade Interlocking nailing has got its own share of indications in properly selected patients without the usual complications which will be evaluated in detail in this study.
MATERIALS AND METHODS This prospective study comprises of 20 diaphyseal fractures in 20 persons treated with Antegrade Intramedullary Interlocking nailing INCLUSION CRITERIA: Closed fracture shaft of humerus. Grade I and II compound fractures. An angulation of more than 15 after closed reduction. Associated neurovascular compromise. Poly trauma. Age more than 17 years when the physis is fused. The fracture line is 3 cms beyond the surgical neck of the humerus and 4 cms proximal to the tip of the olecranon fossa. EXCLUSION CRITERIA: Presence of open physis. Grade II and Grade III compound fractures. Fracture involving the proximal 3cms. and the distal 4cm of humerus. Evaluation of patients: Routine investigations like Haemogram, Blood Sugar, Urea, Creatinine, Serum electrolytes, X-Ray Chest, ECG, BT/CT was done. All the patients were medically fit for anaesthesia and surgery. Radiographic Evaluation: Standard radiographic evaluation of the humerus should include two views taken at 90° to one another, with the shoulder and elbow joints included in each view35.Advanced imaging such as CTis rarely necessary for humeral shaft fractures. It is necessary to carefully examine preoperative radiographs of the involved humerus and assess the canal diameter to decide on the treatment option and avoid any devastating complication in the aftermath.
PREOPERATIVE PLANNING Several variables must be considered before formulating a treatment plan. The fracture pattern, degree of soft tissue injury, associated neurologic injury, patient age, co-morbidity, and patient compliance should be considered together to optimize treatment success and limit the risk of complications28. In all cases, fracture management is combined with early motion and rehabilitation of the injured extremity to limit problems associated with immobilization. The nail size is measured from the radiograph of the normal bone. It is measured between the tip of the greater tuberosity to a point 3cms proximal to the tip of the olecranon fossa. The best method is by use of a scanogram where the nail of approximate length is tied to the normal arm and a radiograph is taken20. Accurate assessment of canal diameter is imperative in the preoperative plan for the following reasons: (1) the humerus does not tolerate reaming well, (2) some nails are available in only one size and (3) excessive reaming may have potential drawbacks (i.e., cortical necrosis), and certain types of nails are more prone to complications when small-diameter nails are used7. In spite of the pre operative planning we have to keep ready the whole range of the nail system.
SURGICAL PROCEDURE The patient is placed on a beach chair or similar reclining support. The patient is then brought to the edge of the radiolucent table and a roll placed underneath the scapula. The shoulder should easily extend to 30° to expose the humeral head from beneath the acromion. The C-arm may be positioned in one of three ways most convenience: (1) on the unaffected side of the patient, (2) at the head of the patient with the C-arm moved parallel to the humerus, or (3) perpendicular to the patient on the affected side with the swing of the C- arm in line with the patient12. The arm is prepared and draped free in the sterile field. Anteroposterior views of the humerus are obtained with the arm anatomically positioned. Gentle rotation can also be used to project a lateral view. A graduated ruler may be positioned on the arm to determine the appropriate length of nail required. Approach:The antegrade approach is commonly used for fractures involving the proximal and middle thirds of the humerus; however, distal third fractures can also be treated with antegrade humeral nails. The incision is typically made anterolateral to the acromion29. Lateral or posterior placement of the incision increases the risk of fracture of the proximal end of the humerus on nail insertion. A deltoid-splitting approach is used, and the subdeltoid bursa is exposed and excised to visualize the supraspinatus tendon. The deltoid should not be incised farther than 4 to 5 cm distally to avoid injury to the axillary nerve. The supraspinatus tendon is incised in line with its fibers with the arm adducted and flexed across the chest. The entry portal is based just medial to the greater tuberosity. The potential drawback with a lateral portal is that the lack of linear access to the humeral canal necessitates additional medial tearing of the rotator cuff as the nail is inserted38. This can be seen per operatively as a depression of the anatomical neck. The entry point can also be checked by image intensifier. After nail placement, care must be taken to repair the supraspinatus tendon. The incision for the distal locking screws is based lateral to the biceps tendon. The tendon is retracted medially, with care taken to protect the branches of the lateral antebrachial cutaneous nerve. Injury to the anterior interosseous nerve may also occur during anteroposterior insertion of distal interlocking screws in the antegrade approach. These injuries are usually transient and resolve in a period of weeks to months. Reduction: Fracture reduction can be accomplished with gentle longitudinal traction and manual manipulation38. However, excessive traction and manipulation increase the risk of neurologic injury. Entry portal: Through the image intensifier the entry point which is just medial to the greater tuberosity and in the area at junction between the articular surface of the head and greater tuberosity is marked with k wire. An awl is introduced over a previously marked K wire site. This starting position is directly in line with the intramedullary canal but should be confirmed by fluoroscopy4. Reaming: Intramedullary reaming can be used to facilitate insertion of the selected nail. This prevents the development of hoop stresses at the entry point while insertion of the nail. When reaming is chosen, it must be ensured that cortical contact at the fracture site is achieved before passage of the reamer. Cortical fracture gaps place the radial nerve at risk of injury when the reamer is passed across the fracture. Unreamed nails must be passed by hand or very gentle tapping. However frequently reaming before nail insertion significantly increases muscle and surrounding soft tissue blood flow when compared with unreamed nails and that this increase persists for up to 6 weeks. An increase in blood flow to the soft tissues may also improve cortical blood flow6. Studies have demonstrated increases in cortical blood flow up to five times control after reamed nailing. The degree of reaming may also be important in optimizing patient outcomes. Also in fractures that compromised circulation (i.e., segmental fractures), limited reaming led to the smallest degree of cortical porosity when compared with standard reaming or controls. Proximal nail care: It is important to ensure that the proximal end of the nail is buried within the substance of the humeral head to limit shoulder impingement. Locking screws: Distal fixation can be achieved by interlocking screws or interference fit. To ensure rotational stability, screw fixation is recommended at each end of the nail to control rotation. Under image guidance the location of the distal locking slot is noted and a stab Incision is made on the anterior aspect of the arm. Both the biceps and the brachialis are split to reach the anterior surface of the Humerus. Under image control, the bone is drilled using 2.9mm drill bit and distal locking is achieved using 3.9mm screw passed anteroposteriorly for 7mm nail and 2.5 drill bit, 2.9mm screw used for 6mm nail.. Distal locking can also be achieved by using a distal locking jig. In contrast to the laterally based distal locking screw fixation in femoral and tibial nailing, humeral nails are distally locked in either a posterior-to-anterior (safest in terms of nerve proximity), anterior-to- posterior, or lateral-to-medial direction40; however, the difficulty in placing most multiply injured patients in the prone position limits use of the posterior-to-anterior approach. When the lateral approach is used, care must be taken to use blunt dissection to bone to ensure that the radial nerve is away from the drill. The fracture site can be compressed by back slapping the nail after insertion of the distal locking screw. The Proximal locking is achieved by using 3.9 mm self-tapping locking screws. This is applied by using the jig and the screw is passed lateral to medial. Care has to be taken to avoid the axillary nerve, which is situated on an average 4.56cms distal to the acromion11. The screw slot can be predrilled with 2.9mm drill bit. The rotator cuff has to be repaired using a non-absorbable suture. All the wounds are closed in layers. Suction drain must be kept inside the shoulder joint.20
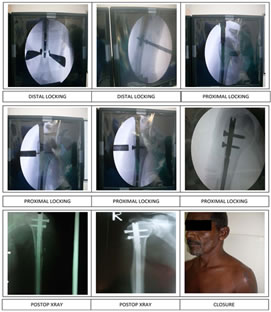
Figure 1: PROCEDURE
POST OPERATIVE TREATMENT Intramedullary interlocking nailing is done with the aim of providing early active mobilization of the limb. Drain tube is removed 48-72 hrs after the surgery. Antibiotics are given up to the fifth postoperative day. Patient is taught passive and active range of motion exercises and he is made to perform the same as the pain permits. This includes pendular motion exercises and the supported and active abduction exercises involving the shoulder and flexion exercises involving the elbow. Progressive increasing weight bearing can be promoted with time. Serial radiographs are taken at monthly intervals in two perpendicular planes to note for the fracture union. Figure 1: PROCEDURE Intramedullary interlocking nailing is done with the aim of providing early active mobilization of the limb. Drain tube is removed 48-72 hrs after the surgery. Antibiotics are given up to the fifth postoperative day. Patient is taught passive and active range of motion exercises and he is made to perform the same as the pain permits. This includes pendular motion exercises and the supported and active abduction exercises involving the shoulder and flexion exercises involving the elbow. Progressive increasing weight bearing can be promoted with time. Serial radiographs are taken at monthly intervals in two perpendicular planes to note for the fracture union. Figure 2
FOLLOWUP ASSESSMENT RODRIGUEZ MERCHAN CRITERIA32 As in most studies of humeral shaft fractures, in this study fracture union, shoulder joint function, and complication and reoperation rates were used as outcome criteria. In a series of radiographs, absence of signs of union 6 months after the injury is generally regarded as nonunion.
Table 1
Restriction in shoulder joint ROM of less than 5–10 degrees in any direction has been used as a criterion of a good functionalresult in previous studies of humeral shaft fractures. Only a few investigators have used shoulder scoring systems (McCormack et al. 2000, Scheerlinck and Handelberg 2002). These scores take into account pain, restriction in ROM in every direction and loss of strength and thus better reveal any problem arising from the shoulder joint than ROM alone. The uninjured side was used as a control in every measurement to compensate for the wide variability of shoulder joint mobility and strength between different individuals. It is possible; however that fracture site pain interferes with pain originating from the shoulder joint. Shoulder joint pain often radiates to the deltoid insertion in the proximal humeral shaft and it may be impossible for the patient to tell the difference between these two types of pain. The basic goal of management of diaphyseal fractures of humerus is to achieve union and restore good function. While assessing results of this study more stress was given to functional recovery and early return to the prefracture state. Union of the fracture was judged clinically by the lack of pain or tenderness at the fracture site and by assessing serial radiograms for presence and consolidation of the bridging callus1 Table 2
The results were studied using the Rodriguez Merchan criteria with due consideration given to shoulder and elbow functions as far as the pain and range of movements are concerned. Only 5% of the cases got poor results and excellent results were achieved in 35% of the cases indicating the usefulness of the procedure. DISCUSSIONThere are several modalities for the management of diaphyseal humeral fractures. Isolated, low energy humeral shaft fractures usually can be treated satisfactorily with non-operative methods but operative stabilization often is necessary for acute, high energy humeral shaft fractures to improve healing, fracture alignment, and functional results9.Although plate osteosynthesis can afford a rigid fixation and good functional recovery, its disadvantages like requiring a wide surgical exposure and more time when compared with intramedullary fixation has been reported15. Interlocking nail gives rotational stability, decreases the need for postoperative bracing and allows early mobilization of the extremity6. Locked intramedullary nails usually can be inserted using closed techniques, avoiding the extensive soft tissue dissection required for plating.A series of 20 cases of fracture shaft of humerus treated by antegrade intramedullary interlocking nailing were studied. The results of the use of intramedullary nailing for the diaphyseal fractures of the humerus have been mixed, with some studies showing good outcome and some others poor outcome. In our study most of the patient’s age was between 40 to60 years.Also high energy trauma was responsible for the majority of injuries in young patients, and this is the population that most of the orthopaedic literature focuses on4.Most of the cases in our present study (75%) were following a road traffic accident indicating the enormous implications this epidemic on the health care resources. 6 cases had associated injuries in our study. In our series of 20 cases careful history taking and thorough clinical examination as per the set standard protocols helped us in proper selection of cases and meticulous preoperative planning resulting in lesser complications. In our series union was noted in 18 of the 20 cases (90%) of fracture humeral diaphysis. Ingman and Waters in 1994 reported union in 95%. Ikpeme in 1994 published 100% union in his study20. Crates and Whittle, in 1998 had a 94.5% unionrate10. Our study is comparable to other international studies, which mention a union rate of 90 100%5, 9, 10, 28.On the other hand plate osteosynthesis gives a fracture union rate of 93 – 100%15, 31, 42 while functional bracing for the humerus show a union rate of 97-100%30, 41, 42.The average time for union in our series was 15.4 wks. (14 – 18) wks for all acute cases. This is comparable to series by Rommene et al., 1998, which showa union time of 12.3 wks to 16 wks1,11,22 In our study, 10 %( 2) cases showed nonunions at the end of24 weeks. This is comparable to study of Rommene et al. in 199838 which show 7.4% non-union. All the cases in our series were fixed with closed interlocking nailing. The one case with non-union was addressed with open reduction and bone grafting with antero lateral approach. This has accounted for the nil incidence of radial nerve palsy. Even in cases of iatrogenic nerve palsy reported in the literature90 percent of these palsies are neurapraxias and the patient recovers spontaneously. The onset of recovery usually occurs within 3 months but can be delayed up to 6 months. The risk for injury to the radial nerve usually is during reaming and nail insertion. Somatosensory evoked potential (SSEP) monitoring during closed humeral nailing has been reported to be useful in accurately identifying neurologic problems that necessitate a change in the surgical plan5. Radial nerve injury can be minimised by avoiding excessive traction and fracture manipulation during the surgicalprocedure.13 However in our series none of the cases presented postoperatively with axillary nerve palsy.All nails in our series were locked with one or two distal locking screws for stability. Given the proximity of important nervous structures, their variable position, the varying position of the tip of the nail, and the lack of any clearly visible or palpable landmarks or “safezones,” percutaneous insertion of distal locking screws through “stab” incisions are dangerous. The median nerve, musculocutaneous nerve (and lateral cutaneous branch), and brachial artery are at risk from the anteroposterior approach1. Difficulty was noticed in the insertion of the distal locking screw due to the sloping contour of the anterior surface of the distal humerus. This was further complicated by the muscle bulk of the biceps and brachialis, which interfere with the distal locking mechanism. In our study 4 of 20 cases (20%) had shoulder problem which is comparable to Ikpeme, 1994 et al.20 (20%) and Crates and Whittle in 199810(13.7%).In our series, 16 of the 20 cases (80%) of the fracture of shaft of humerus attained near normal range of motion of the shoulder joint. It was observed that the movements and the functional ability of the shoulder depended upon the amount of consolidation at the fracture site, and the rehabilitation programme used. These findings are comparable to those of other studies, which show a 90 – 95% return of shoulder tonormalcy5,10,28Proximal protrusion or inadequate insertion of nails may cause subacromial impingement and shoulder pain. Inadequate insertion of nail in one case in our present series ended with severe shoulder joint symptoms. The impingement at the shoulder joint can be overcome by impacting the nail deep into the bone before locking the nail. In our series none of the case developed restricted elbow movements. In antegrade insertion technique since the triceps mechanism is least involved there was no restriction in the range of motion of the elbow. In our study one case (5%) developed superficial wound infection that healed by antibiotics, which is also consistent with other international studies28. This can be attributed to the lesser exposure time, smaller incision and lesser bulk of implant being used. Post op mobilization of the shoulder and elbow was very critical in attaining the amount of movements of the shoulder. Better results were noted in more educated rehabilitation program, with an active involvement of the patient. The results of the criteria correlated well with functional ability of the patients. It takes into consideration all aspects of the fracture complications including shoulder range of movements, elbow movements, pain in the shoulder and the functional disability.CONCLUSIONLocked intramedullary nailing is a novel treatment option for diaphyseal fractures of the humerus. It is ideal in treating diaphyseal fractures of the humerus in patients when other treatment methods are likely to fail, like those with osteoporosis, severely comminuted segmental fractures and polytrauma where reduction in operating time and early rehabilitation are the primary objective. The concept of biological fixation in terms of unreamed nailing, closed reduction, static locking, and fracture site compression promotes early and adequate fracture union. The problem of shoulder impingement and peri-arthritis shoulder can be reduced by placing the nail flush with the bone at the entry site, adequate repair of the rotator cuff, and by educated motivated rehabilitation program, which promotes good functional outcome. Despite some methodological limitations, this study gave useful information and solutions to handling of specific problems associated with antegrade IM nailing of humeral shaft fractures. Antegrade nailing should be avoided in patients with preexisting shoulder pathology or those who will be permanent upper extremity weight-bearers (para- or quadriplegics). Locking of the nails should be done both proximally and distally with screws. Use a mini-open technique for distal locking. Intramedullary nailing in narrow-diameter canals should be avoided. Excessive reaming is not desirable in the humerus. Nail length should be chosen carefully and it may be errored on the shorter side rather than the longer side. Do not distract the fracture site by trying to impact a nail that is excessively long. Locked intramedullary-nailing is an effective and safe alternative for the treatment of diaphyseal humeral fractures. It is suitable for treatment in patients with osteoporosis, pathological fractures, polytrauma and associated neurovascular injuries. It helps in providing early rehabilitation and lessens the morbidity.REFERENCES
Policy for Articles with Open Access:
|
|

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.