 Home
Home|
Table of Content - Volume 15 Issue 1 - July 2020
Role of MRI to assess the progress of spinal tuberculosis during the course of treatment
Saurabh Dwivedi1*, Chandra Prakash Pal2, Yogendra Kumar Mishra3, Tanu Mishra4
1Resident, 2Head Of Department, 3Resident, Department of Orthopaedics, SN Medical College Agra, Uttar Pradesh, INDIA. 4Resident, Department of Radiology, RML Lucknow, Uttar Pradesh, INDIA. Email: dwivedi7500@gmail.com
Abstract Background: Spine is the commonest site of skeletal involvement in tuberculosis and constitutes more than 50% of all forms of osteo-articular tuberculosis. MRI is the most valuable non-invasive diagnostic and prognostic tool in the patients with spinal tuberculosis to promote early detection of disease and assess the response of treatment and change in regime of A.T.T. accordingly. Objective: Magnetic Resonance Imaging pattern of Spinal tuberculosis during course of treatment, to promote early detection of spinal tuberculosis and assess the response of treatment and change in regime of A.T.T. accordingly. Material and Methods: In this study, the MRI scans of 49 consecutively managed spinal tuberculosis patients with or without neurological deficit over 1.5 year period were studied cross-sectionally in the Department of Orthopaedics, S. N. Medical College, Agra were analyzed, to determine the pattern of occurrence of various pathological lesions. They were followed up with anti-TB treatment (ATT) according to standard guidelines. Result: It was found that spinal tuberculosis was most commonly observed in the 31-50 years age group with a male predominance. The dorsal and the lumbar vertebrae are commonly involved and multiple vertebrae were often affected with kyphotic deformity in 36% cases. Intervertebral disc involvement with pre and paravertebral collections were commonly seen in about 75 % of the cases. Cord oedema was noted in 20% of the cases. Nerve root compression was seen in 63% of cases. Thirty-five patients had no neurological deficits while 14 had paraplegia of varying severity. The canal encroachment was observed in 75% cases. Serial MRI were done during the course of treatment to assess the disease progression. Conclusion: This study showed that MRI is the most valuable investigation in the evaluation of spinal tuberculosis. The MRI scan is highly sensitive in the detection of various pathological conditions of spinal tuberculosis and their pattern of occurrence. Serial MRI scans can be used to assess the disease response to treatment. Key Word: spinal tuberculosis.
INTRODUCTION Tuberculosis is a chronic granulomatous disease caused by infection with Mycobacterium species. Spine is the commonest site of skeletal involvement in tuberculosis and constitutes more than 50% of all forms of osteo-articular tuberculosis in India. Annually about 6 million people become ill with tuberculosis and two million die from disease worldwide.1 In the developing countries, the disease has an aggressive course, particularly in children and young adults resulting in abscess formation. Consequently, neurologic complications and spinal deformities are frequently observed2. Spinal involvement occurs in less than 1% of patients with TB3,4 but the increasing frequency of TB in both developed and developing countries has continued to make spinal TB a health problem.3,5 Spinal tuberculosis is the most common as well as the most dangerous forms of skeletal TB and accounts for about 50% of all cases of skeletal tuberculosis. Although the dorsolumbar spine seems to be the most common site of the spinal column involvement in spinal tuberculosis, any part of the spine can be affected. Furthermore, the incidence of neurological complications in spinal TB varies from 10% to 44%4. Paraplegia may develop in 20 – 25% cases5. Tuberculosis of spine is the most common cause of non-traumatic paraplegia in the most parts of world. Conventional X-rays are useful in diagnosis of spinal tuberculosis but their main disadvantage is that more than 50% of bone has to be destroyed before a lesion can be seen on a plain radiograph, a process which takes nearly six months. Advanced imaging techniques like Magnetic Resonance Imaging (MRI) make the early diagnosis of spinal TB easier and a considerable number of patients with spinal TB are diagnosed earlier and treated before significant neurological deficits develop. However, patients can still present late with considerable spine deformity6. MRI because of the lack of ionizing radiation, high contrast resolution, ability to detect marrow infiltration and ease of assessment of extradural disease and status of spinal cord, has become the established optimal imaging technique in the diagnosis of spinal infections and their sequel. However, to date, differentiating tuberculous spondylitis from pyogenic spondylitis is a challenge, in view of varied presentation of the former. MRI has the ability to provide excellent contrast resolution in all planes, making the diagnosis and evaluation of tuberculous spondylitis and para-vertebral extension easier. Serial MRI examinations can be used to assess the response to treatment7,8 and are very useful in the management of multilevel infection. Serial MRI scans can also be used to assess the healing of infection.
MATERIALS AND METHODS A hospital based cross sectional study was evaluated. These cases were from the OPD and IPD from the Department of Orthopedics and the patients who were referred to the Department of Orthopaedics from Department of General Medicine, Pulmonary Medicine and Paediatric Department of S.N. Medical College, Agra on the basis of their clinical presentation over a period of 17 months from November 2017 to May 2019 who were fulfilling inclusion criteria. The inclusion criteria of study was those patients aged 21-60 years of age with or without neurological deficit at spinal level with strong clinical suspicion of spinal tuberculosis. A detailed history along with complete clinical examination and laboratory investigations will be done before the MRI examination. Forty-nine patients with paradiscal spinal TB lesion, with/without paraplegia, aged over twenty years were enrolled. All patients having classical clinico-radiological diagnosis of spinal tuberculosis or who showed evidence of healing on treatment or with a proven histopathological/bacteriological/cytological diagnosis of TB spine were included in the study. The cases were (A) freshly diagnosed cases of TB spine and (B) patients who had completed treatment successfully and had a pre treatment MRI examination. Trauma patients, patients with metallic implants, patients with pacemaker or cochlear implants, patients with isolated intraspinal granuloma, isolated posterior complex involvement, isolated cranio-vertebral junction TB, isolated sacral tuberculosis or patients without a classical clinico-radiological diagnosis were not included in the study. Neurological assessment was performed by Jain and Sinha scoring system6.The radiological diagnosis was made on observations of demineralisation of the vertebra, fuzzy paradiscal margin, reduction or obliteration of disc space, along with one or more of the following findings:- destruction of end plates, wedging of vertebra, obvious kyphotic deformity, paravertebral shadows, anterior scalloping of verterbral body and pre and paravertebral abscess. The aspirate of abscesses (n-9) was sent for Z-N staining, pus culture and PCR. In all prospective patients, MRI was performed pre-treatment and repeated after eight months. Magnetic Resonance Imaging (MRI) examinations were done with 1.5 Tesla Philips Achieva machine using shoulder coil without contrast and the following sequences were taken:-
The following features were assessed by MRI: Compartment of spine involved: Epidural/ Intradural/ Intramedullary/ Multiple Epidural involvement assessed for the following
Intradural/ intramedullary involvement Ethical approval was taken from Institution Ethical committee. RESULTS Table 1: Age and Sex Distribution
Table 2: Regional Distribution of TB Spine
Table 3: Clinical Profile of Patients with Spinal Tuberculosis
Table 4: Extent of Tuberculosis Spine In Various Compartments
MR FINDINGS ON HEALINGAll cases were put on Anti Tuberculous Therapy (ATT) regimen as per Directly Observed Treatment Short course (DOTS) which consisted of daily dosage with Rifampicin [R] (8-12 mg/kg/day), Isoniazid [H] (4-6mg/kg/day), Pyrazinamide [Z] (20-30 mg/kg/day), Ethambutol [E] (13-17 mg/kg/day) and Streptomycin [S] (20-40 mg/kg/day). The healing of the vertebral lesion was recorded on complete resolution of marrow oedema, replacement of marrow by fat seen as a bright signal on T1WI and T2WI and complete resolution of paravertebral collections.On follow-up MRI seven showed complete resolution of cord oedema and neural deficit. Cord atrophy was observed in three cases. The other some cases developed cord atrophy on completion of treatment. Demineralisation was seen in most of the cases. Myelomalacia, arachnoiditis, syringomelia, thickened arachnoid complex and meningeal involvement were not found as contrast was not administered for pre-treatment MRI.
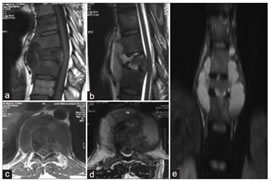
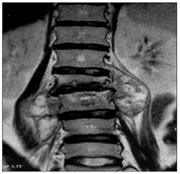
DISCUSSION Tuberculosis has prevailed as a major public health problem especially in our country. Tuberculosis of the spine is clinically important form of extrapulmonary tuberculosis accounting for majority of the musculoskeletal tuberculosis cases. First described in 1782 by Percival Pott, a British orthopedic surgeon usually occurs due to haematogenous seeding of the vertebra from a distant source. Typically, more than one vertebra is involved and usually affects the anterior aspect of the vertebral body adjacent to the subchondral plate and from there on spreads to involve adjacent intervertebral discs. Further with involvement of bone, wedge collapse and vertebral destruction occurs which results in kyphosis (figure2). Epidural abscess formation (figure2) results in narrowing of the spinal canal diameter with resultant cord compression and neurological deficits.In the present study, we have attempted to depict the various spectrum of presentations of spinal TB with clinical correlation. The regional distribution of vertebra in our study was similar to the findings of DJ Kotzke9 and Sajid Ansari.10 Shanley DJ11 evaluated radiographic manifestations of tubercular spondylitis like intraosseous and paraspinal abscess formation as seen in our study mentioned in Figure 1, paraspinal abscesses in the lumbar region gravitate along the psoas sheath(figure 3) which can extend to the femoral region and cause erosion of overlying skin.9,11 MRI is the gold standard of imaging in tuberculous spondylitis due to its superior soft tissue resolution and multiplanar capability. MRI is very useful to see the classic pattern of spread of disease starting anteriorly and moving to opposing vertebrae via subligamentous route. As was observed in our study, T1- weighted images usually show hypointense signal within the affected vertebral marrow. In our study, we had two cases showing intramedullary involvement (Figure 4), on MRI tuberculomas appear as low to intermediate signal intensity on T1W images and low signal on T2W images due to caseous necrosis in the tuberculoma, which has high protein content. The extent of spinal cord involvement, nerve root integrity, posterior elements involvement and also response to ATT therapy are best assessed by MRI. It is important to differentiate tuberculous spondylitis from pyogenic spondylitis because proper treatment of the different types can reduce the rate of disability and functional impairment.12,13 MRI has been shown to be accurate in differentiating tuberculous spondylitis from pyogenic spondylitis. If there are presence of well-defined paraspinal abnormal signal, smooth and thin walled abscess, subligamentous spread of three or more vertebral levels and multiple vertebral or entire body involvement it is more suggestive of tuberculous spondylitis than pyogenic spondylitis.13 Early recognition and prompt treatment are therefore necessary to minimize residual spinal deformity and permanent neurological deficit Early diagnosis and conservative treatment by ATT has shown favorable results as anti- tuberculous drugs will be able to reach the tuberculous caseous material and cavities in spine. However in patients with severe bone involvement along with cord or root compression, surgical treatment is the only benefitable measure.14
Figure 1: |
|


 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.