 Home
Home|
Table of Content - Volume 16 Issue 2 - November 2020
Surgical management of fracture distal end of femur using locking compression plate: A prospective study at BRIMS hospital, Bidar
Anand B Jabshetty1, Vaibhav Bhadbhade2*
1Associate Professor and Incharge HOD, 2Assistant Professor, Department of Orthopaedics, Bidar Institute of Medical Sciences, Bidar, INDIA. Email: vaibhavrb9@gmail.com
Abstract Background: Fracture lower end of femur are unstable, comminuted and tend to occur in elderly osteoporotic or multiple injured patients and hence are difficult to treat. The incidence of malunion, non-union and infection are relative high culminating into potential disability in many reported series. The locking compression plate (LCP) device possesses exclusive biomechanical function that depends on splinting and not on compression, leading to flexible stabilization, quick healing, and reduced bone resorption as blood supply is conserved. Objectives: 1. To study the functional outcome for internal fixation of fractures of the distal end femur by locking compression plate. 2. To evaluate the effectiveness and complications of distal end femur fractures treated with locking compression plate based on rate of union, time till union, rate of infection, varus and valgus mal-alignment and fixation failures. Materials And Methods: A prospective study was carried out over a period of 1 year and enrolled a total of 20 patients with fracture of lower end of the femur. Fractures were classified with the help of radiographs according to the AO-ASIF classification. Reduction of the condyles and fixation were done, and titanium plate was implanted with locking compression screw. Patients were followed up for 9 months and assessed clinically, radiologically, and functionally for functional outcome, fracture healing, and the complications of fracture and surgery. Results: The most common age group was 41-50 years (6), with male (15) predominance. The most common type of fracture according to Muller`s classification was Muller`s type C1 (30%). All patients underwent surgery within 7 days of injury; 90% patients showed radiological union within 18 weeks and 70% patients achieved weight bearing within 14 weeks. Thirteen (65%) patients achieved knee flexion more than 110° and 4 (20%) patients achieved flexion between 90º and 110º . Two patients reveled shortening of 15 mm and one patient showed shortening o 10 mm; 60% (12) achieved excellent while 25% (5) had achieved good functional results according to Neer score. Conclusion: Locking Compression Plate is an important armamentarium in treatment of the Distal femur fractures especially when fracture is closed, severely comminuted and in situations of osteoporosis. Nevertheless, careful understanding of its basic principles and identification of appropriate fracture pattern for use of LCP are essential to prevent complications such as generation of infections and non-and delayed unions. Further study in large number of patients is required to comment regarding disadvantages and complications. Key Words: Fracture of distal end of femur, locking compression plate (LCP)
INTRODUCTION Distal femur fractures exhibit an incidence ratio of about 37 per 1,00,000 person-years1. They occur mainly from two different injury mechanisms. The most common cause is the high impact trauma majorly sustained in road traffic crashes. Intricate knee ligament injuries commonly exist in addition to widespread cartilage injuries. Osteoarthritis may result when there is a diastasis of 3 or more millimeters. These fractures are often unstable, comminuted and tend to occur in elderly osteoporotic of in patients with polytrauma. Because of the proximity of the fracture to the knee joint, regaining full knee motion and function may be difficult. The incidence of malunion, non-union and infection are relatively high in many reported series. These serious injuries have the potential to produce significant long term disability. 2,3 Previously the trend in treatment of these fractures leaned towards closed ,conservative management with traction, casting, or a combination of both. The problem associated with conservative management are the limitation of reduction and difficulty of maintaining reduction. Associated complications of prolonged immobilization and economic considerations of increased hospital stay also limit their utililty . External fixation with devices such as the hybrid external fixator and the Ilizaov external fixator are excellent for the treatment of comminuted fractures associated with bone loss. In addition to maintaining reduction during process of union, these devices can also be used to lengthen the bone. However, pin tract infections and joint contractures are common of these techniques. With the rapid advancements in the arena of orthopaedic surgery, trends in treatment of supra-condylar and inter-condylar femoral fractures now more commonly involves operative management4 . Internal fixation devices that have been used to treat these fractures include the 95º angled blade plate, dynamic condylar screw plate, condylar buttress plate and retrograde supra-condylar inter-locking nail. However, since the complexity of fractures needing treatment has changed from simple extra-articular supra-condylar type to inter-condylar and metaphyseal comminuted types, these implants may no longer be ideal. Double plating, and more recently, locked plating techniques have been advocated5-8. However, with double plating, there is often extensive soft tissue stripping on both sides of the femur, causing reduced blood supply and potential non-union and failure of the implants. The Less Invasive Stabilization System (LISS) allows for fixed angle fixation of the distal femur and minimally invasive fixation of the femoral shaft 9. However, there has been concern that the implant may be too stiff, and when associated with premature weight bearing by the patient, result in ultimate failure of the implant. 10 Internal fixation with LCPs forms a toggle-free, fixed-angle construct. The implant provides numerous points of fixed-angle contact amid the plate and screws in the distal femur, hypothetically decreasing the trend for varus collapse that is seen with the traditional lateral plates. The shaft holes on the distal femoral LCP, which is an additional progress from the less invasive stabilizing system (LISS), are oval enabling for the choices of a compression or a locking screw. This ensures a more accurate positioning of the pate, because it can be compressed closer to the bone8, 11. There have been limited number of studies concentrating explicitly on the LCP condylar plate, out study will aid in defining the role of locking condylar plate in the treatment of distal femur factures. In addition, our study also elucidates the functional outcome for internal fixation of fractures of the distal end femur by LCP and to evaluate the effectiveness and complications of distal end femur fractures treated with LCP based on rate of union, time till union, rate of infection, varus and valgus malalignment, and fixation failures.
MATERIAL AND METHODS A prospective study carried out at BRIMS Hospital, Bidar, Karnataka, India, from August 2019 to July 2020. In our study 20 patients with supra-condylar fracture were studied. The method used for fracture fixation was open reduction and internal fixation with locking compression plate. The duration of follow up ranged 6 months to 18 months.
Exclusion Criteria:
The enrolled patients underwent general, systemic examination and local examination and local examination. Thorough assessment of patient was done to rule out head, chest, abdominal, spinal, or pelvic injury. Evaluation of patients was performed in term of mode of trauma, period between injury and arrival, and musculoskeletal examination of patient to rule out associated fractures. Radiological assessment such as anteroposterior and true lateral views of injured limb including complete knee joint and distal femur/proximal leg was done. Fractures were classified with the help of radiographs according to the AO-ASIF classification. Preoperative Investigation:
Implant Used: The plate and screws are manufactured from 316L stainless alloy with gundrilling technique. The locking compression plates are available from 4 holed to 14 holed. With 4.5 mm thickness plate for lower end of femur. Anatomically pre contoured plate head with soft edges. Locking screw in the head of the plate for a secure support. The head of the locking screw is threaded which gets locked to the plate as it is tightened. LCP combi-holes in the plate shaft gives intra-operative choice between angular stability and /or compression. Preoperative Planning and Preparation: Fractures were classified with the help of radiographs according to the AO-ASIF classification. Preoperative calculation was done on radiographs to ascertain the size of the plate, accurate size of locking, cortical and cancellous screws after subtraction of the magnification factor. The limb to be operated was shaven and prepared a day before scheduled surgery. One gram of second or third generation intravenous cephalosporin was injected previous night and early morning on the day of surgery.
RESULTS In total, 20 patients with fracture of the supracondylar femur were included during the study period of 1 year according to inclusion and exclusion criteria. Gender-wise distribution showed that 15 patients were men and 5 patients were women. As seen in Table 1, the patients were ranging from 22 to 68 years with maximum between 41 and 50years of age, and the median age was 48.6 years. (Table 1) Table 1
16 patients attributed the cause of facture to road traffic accident while 4 suffered a fall. (Table 2)
Table 2
Side of affected limb (Table 3)
Table 3
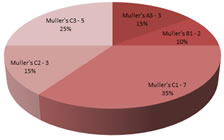
Maximum number of case was of Mullerstype C1-35% (Table 4) and figure 1.
Table 4
Figure 1: Classification of fractures as per Muller`s Classification.
Table 5: shows the time gap between injury and surgery
Table 6: shows union time
Table 7: shows movement of knee i.e flexion in degrees
Table 8: shows functional results according to Neer`s criteria.
DISCUSSION In our study, 20 patients with distal end femur fracture were treated by distal femur locking compression plate. 15 (75%) patients were male. Most common age group affected was 41-50 years with men age 48.6 years. The most common variety of fracture was Muller`s Type C1 (35%). Radiological union was defined as presence of bridging callus across three cortices. Of 20 patients, 19 patients (95%) showed radiological union within 18 weeks, and 14 (70%) patients achieved weight bearing within 14 weeks. The final outcome was assessed in terms of regaining the lost knee using Neers score12. In the study 14 patients underwent surgery within 7 days of injury, and 6 (30%) patients within 3 days of injury. Compared to a study done by Schuta et al..6 internal fixation using the LISS was performed at an average of 5 days (range, 0-29 days) after the injury, which is similar with our study. However, revision operations were required for two cases of implant breakage in that study, while in our study, none of the patients needed any revision surgery. Average follow-up done in this study for each patients was 9 months, and during this time, patients were watched for time of reunion, functional achievement and regaining of work, implant failure, and other complications of surgery. Weight and Collinge13 retrospectively evaluated the use of the LISS-locked plating construct, and nearly, all fractures achieved union at a mean of 13 weeks (range, 7-16weeks) without the need for secondary intervention . On the other hand the study by Kregoret al..5 reported a 93% union rate, without secondary bone grafting, within 12 weeks of surgery. In our study, average time for union was slightly more, i.e., 18 weeks, in contrast with the above mentioned studies; this may be in accordance with the fact that all our cases were treated with open reduction. In the study done by Weight and Collinge13 about 5% nonunion was observed while in our present study, no case of nonunion and only one case of delayed union was found. On analyzing it retrospectively, the reason for delayed union was believed to be owing to inappropriate use of locking screw in place of plan screws. The incidence of infection was about 15% (4), in our study. Which were mainly superficial. The reason for higher incidence of infection were believed to be open reduction and internal fixation treatment. The study by Zlowodzki et al..11 reported deep infection (2.1%), which was not seen in our study. Kregor et al..5 reported implant failure in the form of proximal screw loosening that occurred in 5 cases of 103 patients and each required revision surgery. However, no patient was found to reveal implant failure in our study. Schutzet al.. 6 reported four cases of implant loosening. Kregor et al..5 reported mean range of motion knee to be 1º-109º. However, in present study, all patients achieved good movement with 14 (70%) patients showing knee flexion more than 110° and 4 (20%) patients achieving flexion between 90º and 110°, which is compatible with daily activity. Our study reported that 12 patient showed excellent, 5 good, and 2 fair results, and only 1 showed poor result, while the study by Yeap and Deepak showed that, of 11 patients, 4 patients showed excellent result, 4 good, 2 fair, and 1 failure.
Limitations of Study The use of LCP was not utilized commonly for fracture around knee. This study gives basic data for management of this type of fracture and will help other orthopedic surgeons to manage their patients. The limitations were less patient population and shorter length of follow-up. The study could be extended with recruitment of more patients and a longer period of follow-up.
CONCLUSION Locking Compression Plate is an important armamentarium in treatment of the Distal femur fractures especially when fracture is closed, severely comminuted and in situations of osteoporosis. Nevertheless, careful understanding of its basic principles and identification of appropriate fracture pattern for use of LCP are essential to prevent complications such as generation of infections and non and delayed unions. Further study in large number of patients is required to comment regarding disadvantages and complications.
REFERENCES
.
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Forensic Medicine (Print ISSN: 2579-0935) (Online ISSN: 2636-4735) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.