 Home
Home|
Table of Content - Volume 16 Issue 3 - December 2020
Calceneal enthesophytes (spurs): An observational study on the incidence of spur related heel pain in a tertiary care hospital
M Mahendra Kumar Reddy1*, Chowdam Jagan Babu2, B Someswara Reddy3, B Chandranna4
1Associate Professor, 3Professor & HOD, 4Professor, Department of Orthopaedics, Santiram Medical College, Nandyal, INDIA. 2Assistant Professor, Department of Orthopaedics, Karpaga Vinayaga Institute of Medical Sciences, Palayanoor, Madhuranthakam INDIA. Email: dr.mahendrareddy@gmail.com
Abstract Background: Spur formation is one of the most common cause of heel pain. Heel pain affects daily life of the patients. very few studies have been carried out to find the incidence of spur related heel pain in India. Aim and objective: To study the incidence of spur related heel pain in a tertiary care hospital Methodology: Present study was a prospective study conducted on patients coming with complaints of heel pain. Total 200 patients were studied. Data collected was demographic data, clinical history and clinical examination. Diagnosis of spur was made with X-ray ankle lateral view. Data was analysed with appropriate statistical tests. Results: Overall incidence of spur in the study population was 62%. The incidence of spur was high in females (73%) than males (51%). Chi square was applied and we found that the difference was statistically significant. (p<0.05) Most common age group with spur was 41-50 years 46(37.1%) followed by 51-60 years 31(25%). Most common type of spur was plantar spur 77 (62.1%) followed by combined spur 30(24.19%).
INTRODUCTION Heel pain is one of the most common complaints in patients presenting to orthopaedic department. Prevalence of the heel pain was observed in 10-15% of adults.1 Most common complaint of the patient was pain upon initiation of weight bearing especially on rising in morning or after period of rest. Pain decreases after few minutes and it again returns as the day progresses or weight bearing is for prolonged time. Along with heel pain other observed symptoms are tightness of the Achilles tendon, pain upon palpation of the inferior heel and plantar fascia, inappropriate shoe wear and increased Body Mass Index.2-5 Most common cause for plantar heel pain is biomechanical stress of the plantar fascia and its enthesis of the calcaneal tuberosity. Repetitive traction of the insertion of the plantar fascia into calceneum and vertical compression leads to inflammation of reactive ossification of enthesis. It results in spur formation. 6-9 The reasons for heel pain include Plantar fasciitis, Achilles tendinitis, calceneum fracture, atrophy of heel pad enlarged calcaneal spur and neurological conditions affecting the nerves near ankle. Most commonly heel pain is associated with spur. 10 Various studies observed incidence of spur formation ranging from 15 %-55 %. 11-13 very few studies have been carried out in India. Spur can be diagnosed with clinical history and Xray ankle lateral view. Knowledge of the age and sex incidence and risk factors associated with spur formation will be helpful for prevention of spur formation and progress of the disease. Present study was conducted to study the incidence of spur related heel pain in patients attending tertiary health care centre. Aim and objective: To study the incidence of spur related heel pain in a tertiary care hospital
MATERIAL AND METHODS Present study was a prospective study carried out in department of Orthopaedics at a tertiary health care centre. Study population was patients coming to Out-patient department of orthopaedic department with complaints of heel pain. Inclusion criteria:
Exclusion criteria:
Study was approved by ethical committee of the institute. A valid written consent was taken from the patients after explaining study to them. Total 200 patients were studied. Data was collected with pre tested questionnaire. Data collected was demographiv data like age, sex etc. clinical history was noted. patients with old fracture ankle and any traumatic pathology of talar and subtalar joint were excluded. Through clinical examination was done. All patients were investigated with X-ray ankle lateral view. Radiological diagnosis of calcaneal spur was made and reported by radiologist. Patients with confirmed diagnosis were included in the study. Data was entered in excel sheet. Data was analysed with SPSS version 20.
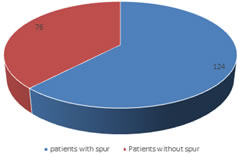
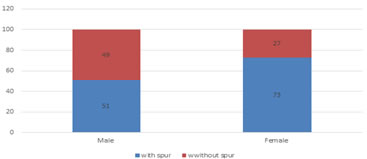
RESULTS Fig 1 shows incidence of spur (Calceneal enthesophytes) in patients studied. We studied total 200 patients, out of these 100 were male and 100 were female. If a patient had spur in both the foot, X-ray of one foot was considered. In our study, out of total 200 patients, 124 patients had spur. Remaining 76 patients complained of heel pain but were without spur. Overall incidence of spur in the study population was 62%. In our study, out of 100 male 51 patients were with spur while 49 patients were without spur. In 100 females 73 had spur and 27 were without spur. Thus incidence of spur was high in females (73%) than males (51%). Chi square was applied and we found that the difference was statistically significant. (p<0.05) (fig 2) Table 1 shows distribution of patients with spur according to age group and sex. Out of total 124 patients 73 were female and 51 were male. Most common age group with spur was 41-50 years 46(37.1%) followed by 51-60 years 31(25%). Patients in the age group of 31-40 years and 61-70 years were 23 (18.55%) and 15(12.1%) respectively. Extremes of age group showed less prevalence. In the age group of 18-30 years only 2 patients were observed. Above 70 years 7 patients (5.64%) were found with spur. Similar distribution was found in both the sexes. Most commonly observed age group in male 19 (37.25%) and female 27(36.99) was 41-50 years. Second most commonly observed age group was 51-60 years in both males and females with 21.57% and 27.45 patients respectively. In the age group of of 18-30 years 2 patients were female, none of them was male. Table 2 shows distribution of patients with spur according to age group and type of spur. Out of total 124 patients 77 (62.1%) had plantar spur. Achiles spur was observed in 17 (13.71%) patients and combined spur were seen in 30( 24.19%) patients. Achiles spur were seen maximum in 41-50 years 7 (41.18%) age group followed by 51-60 years 4 (25.53%). In the age group of 18-30 years Achiles spur was not observed. Plantar spur was observed most commonly in the age group of 41-50 years (40.26%) followed by 51-60 years (27.27%). Patients with plantar spur in the age group of 31-40 years were 16.88%. Combined spur were equally distributed in age group of 31-40 years and 41-50 years with incidence of 26.67%. Patients in the age group of 51-60 years with plantar spur were 20%. In our study, out of total 51 male had spur. Among male patients Achiles spur was observed in 5 (9.8%) patients. Plantar spur and combined spur in male were observed in 60.78% and 29.42% patients respectively. Among the females, plantar spur was most commonly seen in 46(63.01%) patients followed by combined spur in 15(20.56%) patients. Achiles spur in female was observed in 12 (16.43%) patients.
Figure 1: Incidence of spur Figure 2: Incidence of spur according to sex
Table 1: Distribution of patients with spur according to age group and sex
Table 2: Distribution of patients with spur according to age group and type of spur
Table 3: Distribution of patients with spur according to sex and type of spur
DISCUSSION Incidence of spur in the study population was 62% in our study. In a study by Hechmi Toumi et al., they studied 100 patients from 2 to 96 years attending a trauma clinic and found that there was 38% of the population who had a spur.14 Similar to our study, R. Kevin et al. found 59 % incidence of spur in the study population. They studied 200 patients with heel pain. 15 In our study, male to female ratio in patients with spur was 1.43:1. Incidence of spur was high in females (73%) than males (51%). Chi square was applied and we found that the difference was statistically significant. (p<0.05) Similar findings were seen in R kevin et al. where 60 % of the patients with spur were females. 15 In a study by Hechmi Toumi et al., the prevalence of spurs was significantly higher for woman than men in individuals <50 years of age. It was in accordance with our study. 14 In females, excessive compressive forces are acting at the calcaneum due to factors like obesity, pregnancy and footware so spur formation is observed more. In a survey by Frey C et al., 37–69% of women wear high-heeled shoes on a daily basis. 16 These high heels contribute to excessive compressive forces at ankle. Increase in heel height increases impact at heel strike and alters foot biomechanics. 17 In our study, Most common age group with spur was 41-50 years 46(37.1%) followed by 51-60 years 31(25%). Similar distribution was found in both the sexes. Most commonly observed age group in male 19 (37.25%) and female 27(36.99) was 41-50 years. Second most commonly observed age group was 51-60 years in both males and females with 21.57% and 27.45 patients respectively. Thus spurs were less below the age of 30 years. Spur formation is a part of degenerative process resulting in osteophyte formation. 18 They appear in the form of bony growth. Spur takes time to develop and degenerative changes with osteophyte formation are rare in younger individuals.19 Out of total 124 patients 77 (62.1%) had plantar spur. Achiles spur was observed in 17 (13.71%) patients and combined spur were seen in 30( 24.19%) patients. Achiles spur were seen maximum in 41-50 years 7 (41.18%) age group followed by 51-60 years 4 (25.53). In our study, out of total 51 male had spur. Among male patients Achiles spur was observed in 5 (9.8%) patients. Plantar spur and combined spur in male were observed in 60.78% and 29.42% patients respectively. Among the females, plantar spur was most commonly seen in 46(63.01%) patients followed by combined spur in 15(20.56%) patients. Achiles spur in female was observed in 12 (16.43%) patients. Similar to our study, previous study found that Plantar spur seems to be more common than spur occurring at the insertion of achilles.14 In study by Li J, Muehleman et al., it was indicated that the bony trabeculae of spurs are vertically oriented, suggesting that the stresses responsible for spurs formation may be the result of vertical loading. 20 In a study by Cosentino et al. it was found that people involved in standing for long time as part of their professions were more likely to be affected by spur formation. 21 So considering the above factors prevention of spur formation and prevention of progress of spur can be done with lifestyle changes and use of proper footware.
REFERENCES
.
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Forensic Medicine (Print ISSN: 2579-0935) (Online ISSN: 2636-4735) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.