 Home
Home
|
Table of Content - Volume 17 Issue 3 - March 2021
Cross pins for distal tibial fractures in children
B Sreekanth Rao1*, M Venkaiah2, TVG Krishna3, T Zeeshan Muzahid4, GVS Moorthy5
1Associate Professor, 2Assistant Professor,3Associate Professor,4Assistant Professor, 5Professor, Department of Orthopaedics, Bhaskar Medical College and Bhaskar General Hospital, Yenkapally, Telangana, INDIA. Email: bsreerao@gmail.com
Abstract Background: The purpose of this study was to evaluate the use of closed percutaneous cross pins in distal tibia fractures in children. Aims and Objectives: To anatomically maintain reduction and stability. To shorten the duration of above knee plaster. To avoid reoperations and deformity corrections. Materials and Methods: This prospective study was conducted at the Department of Orthopaedic Surgery in Bhaskar Medical College, Yenkapally, RR District, Telangana from July2018 to November 2020. Permission for study was taken from ethical committee of Bhaskar Medical College. Patients included in study for treatment of displaced distal tibia fractures treatment with percutaneous cross pins with K-wires are children between age group of 3 years to 12 years with displaced closed distal tibia fractures with and without fracture of fibula, polytrauma, irritable with head injury, metabolic and neuromuscular fractures, Gustilo type 1 open fractures. Excluded cases were children below 3 years and above 12 years age, open fractures Gustilo type II and type III, undisplaced fractures which can be treated with plaster, maluniting fractures and fractures requiring open reductions. The selected 20 patients residing in and around semi-urban hospital area were treated with in one week of admission and followed up for period of 8 months to one year. Results were assessed based on- Duration of union of fracture. Achieve ease of daily activities by shortening duration of above knee plaster, effective knee exercises, early range of movement, ease of non- weight bearing ambulation. K-wire removal with ease confirming anatomical union without any need to address deformity corrections or reoperations. Results: Fractures united in six to nine weeks, stability was assessed and plaster made below knee by 3rd to 4rth weeks post-surgery. Quadriceps exercises and non-weight bearing ambulation started on second post-operative day. K-wires were removed mean 7th week. No deformities were found, or reoperations required. Conclusion: The study observed less period of hospitalization, minimal cost of k- wires as compared to TENS nails, plates and screws. Less surgical time required, implant removal was with ease and least expenses incurred, early functional recovery with good results. Keywords: Cross pins, distal tibia fractures in children, k-wires.
INTRODUCTION Fractures of the tibial shaft are the third most common pediatric long bone fracture1. Children’s tibia fractures have a great healing capacity due to thick periosteum and good blood circulation. As a result, closed tibia fractures in the growing skeleton will heal rapidly2,3. About 50% of these fractures occur in the distal third of the tibia4. There is no formal classification system for paediatric tibial fractures. These fractures are typically described on the basis of location (e.g., proximal, midshaft, distal) and fracture pattern or by using an eponym (e.g., toddler fracture). In addition to patient age, the location of injury and fracture pattern are the primary determinants of treatment strategy5. Surgical stabilization may be indicated for children in whom acceptable positioning is not maintained after closed reduction, and those who are ten years of age and older6. In the pediatric patient with polytrauma, the tibia is also the third most common fracture site, behind the femur and humerus7. we preferred to use kirschner wires k- wires as they are cheaper pocket friendly to semi-urban patients compared to the expensive TENS, plates and screws, easily available, easily removable. During follow-ups allows ease of re-application, manipulation by wedging of cast. We followed the biomechanical study of the torsional and bending stability of three commonly used pin configurations in distal tibia fracture fixation. This study has shown adequate stability provided by the parallel retrograde pins initiating at the medial malleolus. It is less technically demanding, requires fewer intraoperative radiographs, and minimizes the risk of iatrogenic injury to surrounding structures8.Two, parallel, retrograde, medial to lateral directed pins provide improved stability to a simple, transverse distal tibia fracture when exposed to external rotation forces. External rotation is the most common stress experienced during short-leg casting of the tibia due to the weight of the cast and tendency for external rotation of the foot8.The present study was to access the advantages of using k- wires in treatment of distal tibia fractures in children in semi-urban region. The Principle of 90-90 degrees spread of forces is followed and practiced as far as possible, for a stable construct with cross pins. It is to distribute deforming forces equally in a special plane of 360 degrees; (90+90+9-+90=360). This is achieved by applying K-wires at 90 degrees apart in all three planes: Coronal (as seen in AP view of X-ray), Sagittal (as seen in Lateral view of X-ray) and in Horizontal plane. The final Radiological appearance of placement of K-wires would be the culmination of angles in all three planes. To reinforce the fixation and to reduce stress rising, a second K-wire is places parallel to the first one in both directions.
Figure 1: MATERIALS AND METHODS In the present case series, 20 cases of displaced distal tibia fractures were treated by percutaneous cross pins with k-wire under c-arm. This study was conducted at Bhaskar General Hospital, Yenkapally, Telangana from July 2018 to March 2020 and followed-up till November 2019. Ethical approval was obtained from the Bhaskar medical college Ethics Committee. All the patients were admitted in casualty under Orthopaedics. 20 children selected for study series between age group of 3 years to12 years of whom 14 were male and 6 were females. One case was Gustilo type I open fracture. Five cases fibula was intact. 8 cases had comminuted fracture, one case was treated for rickets. Haematological investigations, screening, paediatric consultation regarding fitness for surgery was taken. Under anaesthesia guided under c-arm 2 k- wires were passed from above the physis from medial side to opposite side of proximal fragment 1.5 to 2cm above the fracture, depending on fracture comminution and stability 2 k-wires were passed 1.5 to 2cm proximal to fracture site from medial side of proximal fragment to lateral side of distal fragment above the physis or distal to proximal fragment lateral to medial side. Reduction and stability checked k-wire cut and bend at 900, dressing done above knee slab applied. First post-operative day started static quadriceps exercises and protected ambulation under supervision was started on second post- operative day. Discharged on 3rd post-operative day. At 3rdor 4rth week check x-rays were taken with ankle in dorsiflexion and plantar flexion to check for stability and reduction of fracture fixation, any angulations or deformities. Slabs were made below knee promoted knee range of movements. At 7th to 9th week confirming fracture union in anatomical position k- wires were removed. Gradual weight bearing was advised for 3 weeks. one case earlier treated for rickets was given walking cast for 3 weeks after k-wire removal.
RESULTS Of total 20 children treated in this series 70% were male and 30% female.75% of the fractures were distal tibia fibula and 25% cases fibula was intact. 40% cases were comminuted distal tibia fractures. 60% were left sided fractures and 8% right sided. 55% were from rural and 45% from semiurban.1% was open fracture and 1% was earlier treated for rickets. 65% sustained RTA, 20% fall from height and 15% sustained fracture while playing. 70% cases operated by 3rd day and 30% by 6th day. 80% cases cast was made below knee by 4rth week and 20% cases at 3rd week 90% cases united by 8th week and 10% by 9th week. 80% full weight bearing by 11th week and 20% by 12th week. Clinical properties such as the radiographic results of the residual deformities were analyzed by Fisher’s exact test. Two cases had 50 varus deformity got remodeled by 6 months. Full weight bearing by 11th week and male sex was found to be statistically significant (p=0.024) Union of fracture by 8th week and fractures with intact fibula was found to be statistically significant (p=0.026) Cast was made below knee by 3rd week and fractures with intact fibula was found to be statistically significant (p=0.03)
Table 1: Distal tibia fractures
Table 2: Distal tibia fractures,50. varus deformity
DISCUSSION Tibia fractures are the most common pediatric lower extremity fracture 9, and the second most common fracture resulting in hospitalization10.The tibia is the second most commonly fractured long bone in abused children 11. Because of its subcutaneous location, approximately 10% of tibial shaft fractures are open injuries, which meaningfully impacts patient evaluation and management 11. Approximately 50% occur in the distal third. Tibial shaft fractures most commonly occur in isolation (70%) and the majority of these injuries result from low-energy rotational mechanisms 11. Two-thirds of pediatric patients with a tibia shaft fracture have an intact fibula12. Complete fractures of both bones are usually caused by high-energy trauma, whereas isolated tibia fractures usually result from torsional forces13,14. Low-energy, rotational tibial injuries often result in spiral fractures of the tibia alone with or without plastic deformation of the fibula or with tibial and fibular fractures at different levels. Tibial fractures with an intact fibula have less of a tendency for shortening but a greater tendency for varus deformity at final healing 15. Most fractures heal in 8 to 12 weeks and return to full activities can be expected in 4 to 6 months 16 . During the first 18 months after a fracture in a child, there may be spontaneous tibial remodeling17. Deformities to the distal tibia tend to be in the coronal plane, perpendicular to the axis of the ankle joint17. The remodeling capacity is determined by the child’s age and the degree of angulation18. There is an asymmetric stimulation of the physis when the tibia grows faster than the fibula19. The deformity is predominantly characterized by a lateral angulation of the tibia with the apex of the deformity at the fracture site. This anatomy implies that the tibial overgrowth results from the stimulation of its proximal growth plate; the fibula does not overgrow and therefore the deformity forms and progresses at the fracture site in the tibial metaphysis20. Although fractures with varus malalignments (of 5° to 13°) completely corrected at the physis, most valgus deformities (of 5° to 7°) were not fully corrected21. Spontaneous bone remodeling after distal tibial diaphyseal fractures in children is often incomplete. The goal of treating these fractures is to obtain accurate reduction and therefore prevent persistent deformities22. Surgical treatment of pediatric tibia shaft fractures has become more common mainly for non-medical reasons, for example, activities in daily living are easier to handle without a long leg cast23,24. For unstable fractures of long bone in children there are different modalities of management, intramedullary nails as this permits earlier mobilization and facilitates optimal alignment24. Elastic Stable Intramedullary Nailing (ESIN) is now commonly used is minimally invasive, with percutaneous placement of the nails. ESIN has been associated with complications resulting from insufficient nail thickness, malreduction during implant placement, and inadequate stabilization of fractures25. The use of external fixation has declined, however, because of recent reports of complications with the technique, including infection, skin necrosis, delayed union, limb overgrowth, and a need for re-manipulation26. Cast immobilization with percutaneously placed Kirschner wires across the fracture site has been reported to add adequate stabilization of unstable tibial fractures in children27. Maintenance of alignment of the tibial shaft using this approach allows early mobilization and callus formation while minimizing infection risks28. Percutaneous pinning is most appropriate for fractures that can be reduced by closed manipulation, such as simple, transverse fracture patterns29.
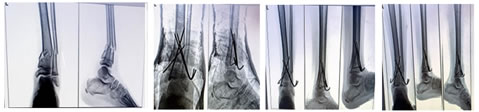
Figure 1: Pre-operative X-Ray; Figure 2: First post-0perative Day X-Ray; Figure 3: Third post-operative week; Figure 4: Seventh post-operative week
Figure 5: Eight post-operative week; Figure 6: Twelfth post-operative week
SUMMARY Tibial shaft fractures are common injuries sustained in paediatric patients. The majority of these pediatric patients go on to uneventful union with excellent final outcomes and return to full activities. Surgical intervention is indicated for fractures that are open, not reducible, have failed conservative management, associated with the compartment syndrome, with polytrauma. Tibia alone provides major rotational stiffness to lower limb. Intact fibula can present difficulty in successful reduction of tibial fractures and have been shown to induce varus deformity if remaining intact30. Closed methods leave the fracture haematoma intact, leading to the formation of early bridging callus.
CONCLUSION Percutaneous K-wire fixation is the biological method of fixation, which provides combination of the elastic stability and mobility. Full weight bearing was seen early among the male patients and cast was made below knee by 3rd week and also union of fracture was seen early among the patients with intact fibula. The study observed less period of hospitalization, minimal cost of k-wires as compared to TENS nails, plates and screws. Less surgical time required, implant removal was with ease and least expenses incurred, early functional recovery with good results.
REFERENCES
Policy for Articles with Open Access
|
|


 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.