 Home
Home
|
Table of Content - Volume 17 Issue 3 - March 2021
Black knee due to alkaptonuria: A case report
Abhijit M Chandge1*, Narendra D Kulkarni2, Nikhil N Avdhoot3
1MS Orthopaedics, HOD, 1,3Department of Orthopaedics, 2Department of Surgery, Dr Hedgewar Hospital, Aurangabad, INDIA. Email: dramhandge@gmail.com
Abstract Background: Black bone disease or alkaptonuria or ochronosis is a rare inborn error of metabolism with autosomal recessive inheritance with a mutation in homogentisate 1,2-dioxygenase. It results in accumulation of homogentisic acid in connective tissues such as, articular cartilage, sclera, skin, tendons and ligaments. Case report: We present a case of 58 yr old male who came to us for severe right knee pain. The physical and radiographic findings were compatible with end stage osteoarthritis. So we planned TKA for him, during which was detected extensive osteoarthritis and brown to black pigmentation of the joint surfaces, the femoral condyles, the tibial Plateau, the menisci and the quadriceps tendon. We report this case as there are very few clinical references in the literature and it is extremely rare for a patient to have undergone total knee arthroplasty with preoperatively undiagnosed alkaptonuria. Discussion: Alkaptonuria usually appears after age of 30 years and is usually asymptomatic until the involvement of the spine, hip, knee and shoulder joints. Hence orthopaedic surgeons must be suspicious of an atypical arthropathy in order to not be overwhelmed during surgery with the presence of darkened cartilage. Keywords: alkaptonuria, ochronosis
INTRODUCTION Alkaptonuria is an extremely rare metabolic disease and is defined as an autosomal recessive inherited deficiency of the hepatic enzyme oxidase of the homogentisic acid. Deficiency of the enzyme causes accumulation of the homogentisic acid in the cells and the body fluids. The disease is characterized by the following three specific conditions, excretion of homogentisic acid in the urine, arthritis and ochronosis. Homogentisic acid accumulates and is polymerized into a blue-black pigment that is ultimately deposited in the skin, cartilage and collagenous tissues. Specifically, pigment deposition can be seen in skin, bones, articular cartilages, ear and sclera, heart endocardium and valves, and kidneys (the so called ochronosis). The accumulation eventually causes severe degeneration of the spine and peripheral joints, like knees, hips and shoulders.
CASE REPORT A 58 year old male presented to us with bilateral knee pain, right knee pain being worse functionally. He could not walk for about 5 minutes and he could not climb stairs No significant information arose from the history as the patient did not suffer from any chronic disease, did not smoke and had no family history of arthritis. On physical examination there was medial joint line tenderness. The range of motion was 5 degree to 100 degree with palpable crepitus. The dorsalis pedis pulse was present. His pre-operative Oxford knee score was 9, while his knee society functional score was zero. Patient had history of hypertension with fresh 2D echo showing calcification of aortic and mitral valve. Old X-ray and MRI of lumbar spine showed narrowing and calcification of intervertebral spaces.
Figure 1: X-ray of right knee showing preop decreased joint space and postop xray after TKA Having failed conservative therapy, total knee arthroplasty was offered and was agreed upon after informed consent. Preoperatively when foleys catheter was tried ,it was not passing into bladder .Hence X-ray was done which showed vesical calculus.Suprapubic catheterisation was done before proceeding to TKA.A midline incision was taken, followed by medial parapatellar approach. Upon everting the patella, it was noted that cartilage over femur and tibia, menisci, cruciate ligaments were black in colour.(Fig 2) With no signs suggestive of infection or malignancy, cemented TKA(smith and nephew) was performed.( Fig 1)
Figure 2: Intraoperaive picture showing black articular cartilage,menisci and ligaments
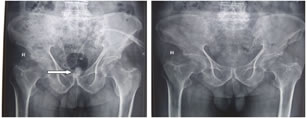
Figure 3: Arrow showing urinary bladder calculus and Xray after stone removal Intraoperative tissue samples were sent for histological analysis which were reported to have deposition of large amorphous brown material in the above structures including synovium, suggestive of alkaptonuria. Subsequent physical examination revealed dark pigmentation of his sclera.(Fig 4) KUB x-ray showed bladder calculus which was removed subsequently by open cystolithotomy.(Fig 3) Figure 4: Pigmentation of sclera and Xray showing calcification of intervertebral disc Post operatively patient was started on physiotherapy as per institution protocol. Sutures were removed after 18 days. {The patient was informed that data from the case would be submitted for publication, and gave his written consent.}
DISCUSSION Alkaptonuria is a rare pathologic condition that is passed as an autosomal recessive trait in most cases,caused by mutations in the homogentisate 1, 2- dioxygenase gene.It occurs in less than 1 in a million births.The first sign of alkaptonuria is often a change in urine color.Darkening of the urine and discoloration of the external ear and sclera may be overlooked by patients and their family members. Therefore, the diagnosis of alkaptonuria may be delayed until ochronosis has developed. Our patient was not conscious of any of these properties until examined .Weight-bearing joints are usually affected in ochronotic arthritis. The knees are most frequently affected, while hip and shoulder joints can also be affected1,5. Signs of ochronotic arthritis may resemble those of rheumatoid arthritis and ankylosing spondylitis.In ochronotic arthritis, small joints usually are not spared. However, osteophytic changes are not as evident as in osteoarthritis. In our case, degeneration of the knee joint was the main cause of the symptom. There is no specific treatment for black knee. Joint manifestations might be mitigable if homogentisic acid accumulation and deposition could be diminished by dietary limitation of phenylalanine and tyrosine. Ascorbic acid prevents oxidation and polymerization of homogentisic acid in vitro, but the efficacy of this form of treatment has not been established.6,9 The usual arthritic drugs and physiotherapy decrease joint symptoms in the early stage of ochronotic arthritis but do not decrease the rate of degeneration of joints. The destruction of the cartilaginous joint surfaces is extensive and appears at a young age, so that the patient requires a total arthroplasty before the age of 60. The total arthroplasty constitutes the unique solution to improve the quality of life for those patients. In our case, the patient mentions dramatic improvement of the quality of life after TKA. As there are no particular contraindications and cases of early loosening of the arthroplasty in literature, the total arthroplasty constitutes the only invasive therapy. The experience we obtained from this case, confirms it.
REFERENCES
Policy for Articles with Open Access
|
|



 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.