 Home
Home
|
Table of Content - Volume 18 Issue 1 - April 2021
Periosteal aneurysmal bone cyst (ABC): A case report
Abhijit M Chandge
MS Orthopaedics, HOD, Department of Orthopaedics, Dr Hedgewar Hospital, Aurangabad, 431005, Maharashtra, INDIA. Email: dramchandge@gmail.com
Abstract Background: An aneurysmal bone cyst (ABC) is a highly destructive benign bone tumor, occurring in less than 1 in 100,000 people per year. The term "aneurysmal" refers to the explosive, expansile nature of the bone containing the aneurysmal bone cyst, similar to the enlargement seen with blood vessel or heart aneurysms. The majority of ABCs are hollow and filled with different sized liquid or blood-filled sacs called cysts. Because ABCs usually are filled with these blood-filled cysts, they are fragile and prone to fracture. Approximately 5% of aneurysmal bone cysts are solid tumors rather than being hollow. Case report: Aneurysmal bone cyst (ABC) is a benign skeletal tumor occurring in first two decade of life in metaphyseal region of long bones. Here we present a rare case of periosteal ABC of proximal tibia in 17-year-old male patient who was treated with excision, curettage of lesion and electro cautery over local cortex to prevent recurrence and stability was provided by tibial plateau plate fixation to prevent pathological fracture. Discussion: Periosteal aneurysmal bone cyst is a rare anatomic subtype that accounts for 16% to 30.3% of all aneurysmal bone cysts. Few cases have been reported in the literature. The approach used to treat these patients is individualized and varies according to the experience of each service. we treated this patient with excision of tumor, curettage, electro cautery application locally and prophylactic plating. It appears that adjuvants can improve local control rate when combined to curettage. The overall local recurrence rate is approximately 12%.
INTRODUCTION ABC is a rare benign skeletal tumor usually occurring in the first two decades of life and typically associated with a growing mass, swelling, pain and bone destruction. Approximately 70% of cases are considered primary lesions and the remaining 30% arising secondary to different primary tumors such as osteoblastoma, giant cell tumor of bone, chondroblastoma, fibrous dysplasia or low-grade intramedullary osteosarcoma. Usually, ABC arises in the metaphysis of long bones like femur tibia and humerus. Generally majority of ABCs are intraosseous, rarely the ABC is localised on surface of long bone. We present a case of periosteal ABC of upper tibia in 17-year-old male patient.
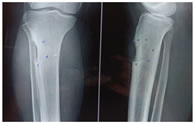
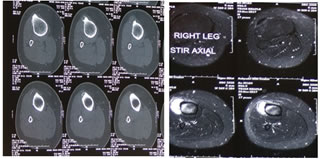
CASE REPORT 17-year-old male patient presented with pain and swelling in right upper third leg since more than one month. On local examination there was swelling, tenderness over lateral aspect of upper third leg. X-ray showed periosteal expansile lytic lesion in metaphysis of right tibia. computed tomography demonstrated a cortical lytic lesion with irregular border in proximal tibia with soft tissue extension which was hyperintense in MRI. First surgical biopsy was done . Histopathological report was ABC.
PREOP XRAY-AP AND LATERAL VIEW OF TIBIA Figure 1
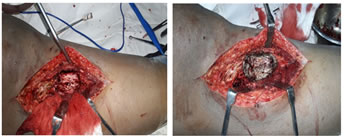
CT SCAN SHOWONG PERIOSTEAL TIBIAL LESION MRI SHOWING PERIOSTEAL LESION Figure 2 Definitive surgical treatment was planned after histopathological report. Anterolateral incision was taken incorporating biopsy site in incision. Tumor was removed from soft tissue and outer surface of upper third lateral aspect of tibia. There was no intramedullary extension of tumor. Curettage was done and then after thorough removal of entire tumor, electro cauterisation of surface area of tumor site was done. Tibial plateau plate was applied laterally. Patient was kept non-weight bearing till two weeks. Sutures were removed after two weeks. Patient was started partial weight bearing for two weeks after suture removal and then was allowed full weight bearing.
INTRAOP PICTURE SHOWING ABC. EXCISION OF ABC Figure 3
AFTER EXCISION OF ABC. AFTER ELECTROCAUTERISATION OF CORTEX. Figure 4
PICTURE SHOWING PLATE. POSTOP XRAY Figure 5
DISCUSSION ABC is a benign but locally aggressive bone lesion, which was once considered a reactive lesion, but now has been proved to have a neoplatic nature characterized by rearrangements of the usp 6-gene.16 Cause of this ABC is unknown. Periosteal origin of ABC is a relatively uncommon finding and has been rarely reported. Periosteal ABCs may exhibit prominent soft tissue component and/or periosteal reaction21. Radiographical differential diagnosis of periosteal ABC include giant cell tumor, telengiectatic osteosarcoma, periosteal chondroma and periosteal chondrosarcoma, chondroblastoma, chondromyxoid fibroma and fibrous dysplasia6,11. Definative treatment for intraosseous ABC is clear in literature15 but not for periosteal ABC. Recurrence rate of periosteal ABC is upto 12%. Optimal treatment method of periosteal ABC is still a matter of debate. In our case we did thorough excion of tumor, curettage and electrocauterisation of involved surface of tibia and applicaton of tibial plateau plate for stability. The rate of local recurrence is reasonably low after curettage followed by other adjuvant procedures.
CONSENT Written informed consent was obtained from patient and his relative for publication of this report and accompaning imaging.
REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Pediatrics (Print ISSN: 2579-0897) (Online ISSN: 2636-4662) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
|


 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.