 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 1 Issue 1 - January 2017
Non union patella with quadriceps contracture – A case report
Rohan A. Bhimani*, Sanjay N. Patil**
*Resident, **Professor and HOD, Department of Orthopaedics, Bharati Hospital, Pune – 411043 Maharashtra, INDIA.
Abstract Introduction: Non union patella with quadriceps contracture is an unusual orthopaedic finding. Very few cases have recorded in the past have been recorded with similar findings. We record a case of 45 year male with non union patella with quadriceps contracture secondary to trauma. Case Report: A 45 year male with post traumatic non union patella with quadriceps contracture since 6months presented in the O.P.D. with complaints of defect in right knee with restriction of movements. The roentogram of right knee confirmed our findings. He underwent Quadricepsplasty with Tension Band Wiring for the patella followed by rigorous physiotherapy to achieve current level of knee flexion of 110 degrees. Conclusion: Thus we conclude that quadricepsplasty with tension band wiring is one the good modalities of treatment for a non union patella associated with quadriceps contracture. Keywords: Non- union patella; Quadricepsplasty; Fracture Patella;Tension Band Wiring; Patellectomy.
INTRODUCTION Fractures of the patella contribute almost1% of all skeletal injuries1. The anterior subcutaneous location of the patella makes it vulnerable to direct trauma. Transverse pattern fracture patella is a common form of presentation in clinical practice. Delayed presentation of displaced fracture of patella is not an uncommon presentation in practice. Majority of the times when such cases present in O.P.D., the fragments are grossly displaced. In addition there are soft tissues contractures like quadriceps, retinaculum, and internal ligaments of the knee joint. There is associated knee joint stiffness and extensor lag in these patients. The major hurdle is to bring the fracture fragments together and restore the extensor mechanism either by bone to bone or bone to tendon union. It is necessary that length of the contracted tissues be achieved so that further flexion of the knee is possible. There are three different schools of thoughts which give management for such fracture presentation. One is to go for conservative management with knee ROM exercises. Other option is to go for one staged procedure in which the proximal fragment is mobilized and fixed with the lower fragment using V-Y/ Z plasty and achieving fractional lengthening. The third option is preoperative traction to the proximal fragment by skeletal traction using pins or Ilizarov method to approximate the fragments and the procedure is done in two stages. We have used one staged procedure in this case and the results are encouraging.
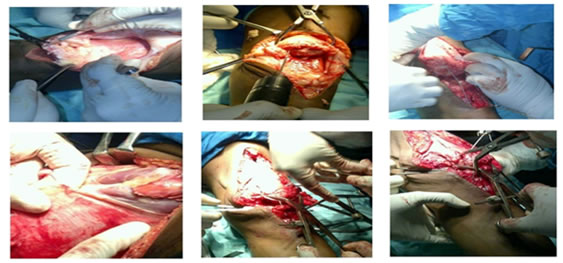
CASE REPORT A 45 year male came to the O.P.D. with complaints of instability and defect in his left knee since 6 months. Patient gave history of trauma due to fall as he was under alcohol influence while walking 6 months back. The patient had not taken treatment for 6 months because of financial constraints and ignorance. On examination, emptiness was present in left knee with intercondylar articulation surface of tibia and femur visible. A swelling was seen in anterior aspect of left distal third thigh, which on palpation was the superior part of the patella. The lower pole of patella was palpable just above the left tibial tuberosity (Figure 1). The radiograph confirmed superior fragment of patella lying in the distal third aspect of thigh and lower fragment close to tibial tuberosity (Figure 2). Patient was then operated by anterior approach where quadricepsplasty and tension band wiring for patella was done after bringing the superior fragment down (Figure 3). Another tension band wire was passed through neutralization hole made just posterior to tibial tuberosity and the retinaculum was then repaired. During Post – Op Period Patient was made to do dynamic quadriceps strengthening exercises and active straight leg raising. After suture removal continuous passive motion for his knee was started. On discharge passive knee ROM was 5 degrees of extension lag to 40 degrees was present. After 6 weeks post operative follow up patient had 5 to 90 degree passive knee ROM. At 3 months follow up patient had knee passive ROM of0 to 110 degrees (Figure 4).
Figure 1: Cinical picture of the patients Figure 2: Roentogram showing fracture affected patella ragment present in of patella with superior f distal third of thigh
Figure 3: intra-operative images of quadricepsplasty, reduction and fixation of patella Figure 4: Post operative x ray, suture line, current x ray and present knee range of movement
DISCUSSION The purpose of reporting this case is to highlight the possibility of the use of single staged procedure in which the proximal fragment is mobilized and fixed with the lower fragment using V-Y plasty and achieving fractional lengthening preventing quadriceps lag in patients of non union of patellar fractures with large gaps between the fracture fragments. The rate of non union in patellar fractures is about 2.4%. There are few cases reported in management of such fractures. All cases of displaced fracture of patella require operative treatment. Patient generally lands up in gap non union because of patient’s ignorance as he can walk full weight bearing. The normal tensile force across a patella is around 3000N which increase up to 6000N in athletes. Patellofemoral compressive forces generated are greater than three times the body weight during routine daily activities and may exceed seven times the body weight while climbing stairs and squatting. These forces only act on the proximal pole if the fracture fragment is accompanied with tears in the medial and lateral expansions. Integrity of the medial and lateral expansions along with anterior fascia lata and sharpies fibers allows active extension of the knee after patellar fracture. Unopposed passage of these forces, as in our case, allows a continuous increase in the gap between the fragments leading to contracture of the proximal quadriceps mechanism. The available support ingliterature on such presentation is as follows:
Table 1: Various Studies Comparing Different Modalities of Treatment for Non Union Patella
The problem with two staged surgeries is that presence of ilizarov or skeletal traction poses a mental trauma to the patient along with surgical complications like bone weakening, pin loosening, pin tract infection and prolong duration of treatment. But two staged surgeries have been reported with good results as shown in the table. We opted for one staged procedure i.e. proximal fragment is mobilized and fixed with the lower fragment/patellar tendon using V-Y/ Z plasty and achieving fractional lengthening. Patellectomyis the most commonly practiced management which is accompanied with problems like long periods of rehabilitation and restricted range of motion. Patellectomy basically compromises the length of lever arm of external apparatus mechanism, thereby causing excessive stress on the knee joint during extension which ultimately causes early degenerative changes and is therefore a relative contraindication for young individuals. The problem with osteosynthesis is the quadriceps contracture which causes separation of the fracture fragments. This was seen in our patient and approximation of these two fragments is very difficult. But we implied the technique of V-Y plasty, which is the commonest practiced technique for such conditions and we also tried this technique with very good results.
CONCLUSION Thus we conclude that quadricepsplasty followed by tension band wiring is a good surgical measure in treatment of non union patella with quadriceps contracture.
CLINICAL MESSAGE Of many techniques available, we believe that quadricepsplasty with tension band wiring is a superior modality of treatment and should be used for patients with such unusual presentation.
REFERENCES
|
|


 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.