 Home
Home
|
Table of Content - Volume 20 Issue 1 - October 2021
Evaluation of high-grade acromioclavicular dislocations fixed by coracoid sling procedure
S Abdul Hameed Ansari1*, M Angathakumar2
1Associate Professor, 2Senior Resident, Department of Orthopaedics, Government Thiruvarur Medical College, Thiruvarur, Tamil Nadu, INDIA. Email: bansarinas@yahoo.com
Abstract Background: To evaluate the outcome of high grade Acromioclavicular (Grade 3 and above) treated by Reconstruction with Ethibond sutures with Coracoid sling procedure. Methods: 22 patients age range from 25 to 50 (mean 38) underwent Acromioclavicular joint reconstruction of Rockwood Grade 3 (n=3) Grade 4(n=11) Grade 5 (n=8) using Coracoid sling procedure with double strand 5 Ethibond sutures. The mean period from injury to procedure was 5.7 days. Outcome was assessed using VAS and DASH scores preoperatively and 3 months after procedure. Results: Out of 22 patients 21 patients had excellent results, and their VAS score reduced from 6.78 to 0.91 and DASH score reduced from 23.4 to 3.78 after 3 months. One patient had mild subluxation of Acromioclavicular joint after one month, but the scores were comparable with other patients Conclusion: Among the biological fixations of Acromioclavicular joint dislocations; this procedure also gives promising results, less demanding and less expensive technique Key words: Acromioclavicular joint dislocations; VAS score, DASH score.
INTRODUCTION Acromioclavicular injuries are common injuries in Road Traffic accidents in Tamilnadu, India. Low grade injuries are usually conservatively managed or neglected but with lesser degree of morbidity only. But high-grade Acromioclavicular injuries are usually fixed or otherwise they go for complications like shoulder stiffness and weakness. It imposes a greater loss to the society when active earning young people were not properly managed. Acromioclavicular high-grade injuries were fixed with either Kwires or Tension Band wiring until recently which ended in complications. Lateral end of clavicle excision has been practiced along with tendon augmentation to balance loss of conoid and trapezoid ligaments. Anatomical considerations: Considering the anatomy of Acromioclavicular joint, the supero inferiorly stability is given by coracoclavicular ligaments, at the same time the ligaments allow anteroposterior rotation.8,910 Acromioclavicular capsular ligament on the other side give anteroposterior stability and allows up to 35degree angle of clavicular inclination during extreme abduction. So Acromioclavicular fixation need to be a dynamic one. Considering this rigid fixation of Acromioclavicular joint which is meant for higher mobility gives the poorer to bad results with implant loosening, stiffness and chronic pain. Hence biological type of fixation is being tried to overcome this especially at the level of Coracoclavicular ligament attachments. In our institution, we tried double stranded ethibond suture material to fix the Acromioclavicular dislocations and did this study. Tsan-Wen et al. have already done the same procedure and published good results.5 Motamedi AR et al. used braided PDS material and did stiffness test and proved the same strength as intact Coracoclavicular ligament complex. Hai-Feng Wei et al. have done study on triple endobutton technique and published good results.11 A study13 of Arthroscopic Weaver-Dunn procedure for Acromioclavicular instability established 90 percent success rate. Classification: Regarding classification of Acromioclavicular dislocations, we followed Rockwood classification. In Type I AC dislocation, joint is well preserved and only strain of ligaments seen. In Type II AC dislocations, complete rupture of AC ligaments and some strain of Coracoclavicular ligaments seen. In Type III AC dislocations, both AC and CC ligaments complete tear seen and 100% displacement of clavicle is seen. In Type IV AC joint dislocations, a type III lesion with posterior displacement of clavicle through trapezius is seen. In Type V AC dislocations, deltoid and trapezius muscle detachment are also seen along with Type III lesions. In Type VI lesions, the clavicle is displaced under the Coracoid process. Ashish Babhulkar and Aditya Pawaskar in their article,12 demarcated the positions of Acromioclavicular ligament, Coracoclavicular ligaments, Deltopectoral fascia and direction of displacement in high grade Acromioclavicular dislocations.
MATERIALS AND METHODS The study was done at Department of Orthopaedics, Government Thiruvarur Medical College from April 2018 to March 2020.Total cases studied were 22 cases. Male cases 17 and Female cases were 5. RTA were 15 and Fall 7 cases. Inclusion and Exclusion criteria: Inclusion criteria were 1) Age between 25 to 50, to rule out age related Shoulder problems in aged individuals 2) Acromioclavicular dislocations of Rockwood type III and above. Exclusion Criteria were 1) Patients with prior history of shoulder problem 2) Patients with head injury 3) Patients with additional same side upper limb injury, chest injury 4) Patients with Diabetes. Preoperative: Immediately after injury, all patients were taken Proper Shoulder AP views after stabilization of general condition. All patients are given pouch arm sling on the side of injury. Additional CT scan shoulder was taken next day to facilitate the typing of the injury. Average time period between injury and procedure was 5.7 days. Visual Analog scale and DASH score are recorded for the side on the day of procedure before surgery. Procedure: All patients were given Interscalene block. Patients are kept in Beach chair position. After draping, a curved incision of about 10cms length with convexity upwards medial starting point one inch below the midpoint of clavicle and lateral end point one inch below and lateral to AC joint with uppermost point of convexity just crossing the posterior border of clavicle. After dissection, temporary fixation of AC joint was done using 2mm K wire in anteroposterior oblique fashion. Then 2 drill holes made in clavicle 2.5cm apart, centering the coracoid process, with 3.2mm drill bit, lateral hole slightly posterior and medial hole slightly anterior. Double stranded 5sized ethibond was introduced through medial hole with the help of Finer crocodile forceps and the blind end routed under the coracoid process with help of right angle artery forceps. Then the suture material taken out from lateral hole with the help of crocodile forceps and knotted over the clavicle. During knotting, temporary Kwire was withdrawn and knotting done with ideal position of clavicle over Coracoid process. Acromioclavicular ligament was sutured with help of 2 ethibond sutures and wound closure done. PostOp: AP view of shoulder to assess the satisfactory reduction, was taken on second post-operative day. Arm Sling pouch applied and Assisted shoulder rising with pouch appreciated after reduction of pain. Shoulder strengthening, forward reaching and shoulder circumduction exercises are appreciated stage by stage. After discharge, patients are reviewed every 15 days. Functional and pain improvement was assessed every time. By the end of 3 months, VAS score and DASH score were assessed and recorded for all patients.
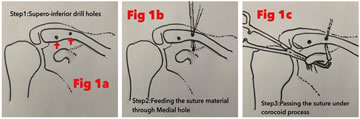
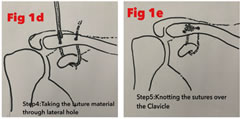
Figure 1a Figure1b Figure1c Figure 1d Figure 1e Figure 1a: Supero-inferior drill holes; Figure1b: Feeding the suture material through medial hole; Figure1c: Passing the suture under corocoid process; Figure1d: Taking the suture material through lateral hole; Figure 1e: Knotting the sutures over the Clavicle Figure 2: Incision line (Patient 10) Figure 3: Knotting over clavicle (Patient 17) Figure 4:Healed incision line and full ROM after 3 month (Patient 5) Table 1: Patients chart
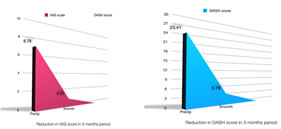
RESULTS In 21 out of 22 cases, the results were excellent and in one case minimal subluxation of the Acromioclavicular joint noted after one month were seen. Even in that case Range of movement was excellent and resultant VAS scores and DASH scores were good. The average preprocedural VAS score was 6.78 and after 3 months it came to 0.91. The average pre procedural DASH score was 23.4 and after 3 months it came to 3.78. Comparing the results of other authors, available in literature, our results are comparable and promising. Table 2: Results
Graph 1 Graph 2 Graph 1: Reduction in VAS score in 3 month period; Graph 2: Reduction in DASH score in 3 month period
Variety of successful Acromioclavicular joint reconstructions are available in literature. According to Vinodkumar et al.3, Surgilig synthetic ligament fixation gave good results comparing the Modified Weaver Dunn procedure. Autogenously Semitendinosus tendon graft was used and gave good results in a study by Galal Mansour Hegazy et al.4 Mohamed Taha El Shewy and Hatem El Azizi7 used double stranded Ethibond sutures for acute Grade IV and above Acromioclavicular dislocations and have published good results.
DISCUSSION High grade Acromioclavicular dislocations pose a bigger burden to society, since it majorly happens in the bread earning age group especially when either conservatively managed or fixed with rigid fixation. Authors of various studies 14 strongly suggest surgical treatment of either open or arthroscopic reconstruction in young individuals. Biological fixation gives a good solution to the Acromioclavicular joint dislocations which do need more flexibility even after fixation. Modified weaver Dunn procedure1 and Luggage tag technique2 are the recent successful techniques that restore the Coracoclavicular stabilizing system which gives supero inferior stability under cyclic loading. But in South Indian population clavicle and coracoid processes are relatively thin structures which may not permit large hole drillings needed in these procedures. In our study, we included a procedure which was technically non demanding and economically less requiring and needed a maximum of 3mm drilling. And at the same time gave almost equal results. This may be due to the thinner build of the South Indian population especially in our area. The patient who had mild degree of subluxation in follow up, was more muscular, proved this also.In their article, Tsan-Wen Huang et al. have postulated that this kind of suspension suture augmentation works as a Suspension bridge model which prevents the redislocation by transforming the deforming forces5
CONCLUSION The study proved the procedure is a successful one. At the same time long term follow up, Stress testing, comparison studies needed to be added to protocolize the study.
REFERNCES
Policy for Articles with Open Access
|
|

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.