 Home
Home
|
Table of Content - Volume 20 Issue 1 - October 2021
Comparative study between dynamic compression plating versus interlock nailing in treatment of fracture of shaft of humerus
Yogendra B Nehate1, Rajendra Hanumandas Agrawal2*
1Senior Resident, 2Assistant Professor, Department of Orthopaedics, Government Medical College Jalgaon, Maharashtra, INDIA.
Abstract Background: To study management with interlocked nail in treatment of acute fracture shaft humerus and to compare its effectiveness with well-established method of plate fixation. Material And Methods: 44 patients with acute shaft fracture humerus treated from August 2004 to August 2006. Out of these 44, 22 patients were treated by plating and 22 were treated by antigrade interlock nailing. Patients were followed for minimum period of 8 months in terms of radiological union time, amount of blood loss, duration of surgery, functional outcome, radial nerve recovery and complications such as infection, iatrogenic nerve palsy and delayed union and non-union. Functional outcome was determined using American Shoulder and Elbow Surgeon's Score. Student’s ‘t’ test was used for statistical analysis and 'p' values were determined. Results: Lock nailing had significantly shorter operation time and blood loss than did plate fixation (58.4 versus 103.8 minutes and 31.5 versus 107.2 ml respectively). Union rate and time to union were not significantly different in both the groups. In the nailing group 3 cases had impingement and one non-union. The plate group had 2 non-unions. There was no significant difference as per radial nerve recovery period concerned. Functional recovery was essentially the same in both groups at 8 months. Conclusion: For treatment of humerus shaft fracture both nailing and plating provide predictable methods for achieving fracture stabilization and ultimate healing. However, Humeral locked nailing offered more advantage in turns less invasive surgical technique, less blood loss and less operation time.
INTRODUCTION Time waits for none and so moves the traffic, adding to the number of trauma per day, Fractures of shaft of humerus also shows a corresponding increase in proportion and young adults usually males are affected more. Due to the involvement of productive population of country, it leads to greater economic loss of country. Most of humerus diaphyseal fractures heal with appropriate care, although a small but consistent number will require surgery for optimal outcome, which is usually suitable, to isolated fractures.1 Most of the early methods of treatment focused primarily on comfort and patient mobilization. The simplest method involved binding the extremity to the patient's body with Sling and Swathe device. Although this did provide comfort and promote union, alignment was poorly controlled. The hanging arm cast, introduced later, achieved better alignment. This method relied not only on a direct splinting effect from plaster but on gravity to overcome the deforming forces. Using rigid plastic orthosis with adjustable straps popularized as functional cast bracing by Sarmiento has given excellent clinical and radiological outcome in fracture humerus.2-4 Although complications are infrequent, nonoperative treatment requires a long period of immobilization, which carries a risk of prolonged shoulder stiffness and may be inconvenient to patient.5,6 Furthermore nonunion after conservative treatment of these fractures does occur in upto 10% of the cases and treatment of this condition can be very difficult.7-9 So there is growing interest in treating even simple humeral shaft fractures by dynamic compression plating or intramedullary nailing in order to avoid these problems and to allow earlier mobilization and rapid return to work.5,10 Due to increasing incidence of polytrauma in today’s era the current emphasis focuses on defining the incidence and health care resources required to treat these patients refining the indications for surgical intervention, decreasing the surgical failure rate through new implants and techniques and minimizing the duration and magnitude of disability post injury.11-13 Various implant options are available for treating humeral diaphyseal fractures e.g. interlocking nails, dynamic compression plating, limited contact dynamic compression plating, flexible nails, locking plates. Compression plate fixation techniques as developed and refined by the AO/ASIF group14 have been shown to be effective in most indications for internal fixation of humeral shaft fractures.10,15,16 Most of the studies have documented the generally good outcome that occurs after compression plating.10,15-19 Furthermore, literature also supports the fact that range of motion of the elbow and shoulder of the involved extremity returns predictably after plate fixation.10,15,16,19 The techniques of interlock nailing represent a newer approach to treatment of humeral shaft fractures. These newer device have demonstrated fewer mechanical problems, malunion, infection, iatrogenic radial nerve palsy, less operative time and blood loss as shown by many studies done in past.20-22 In the present study, we compared and studied the results of treatment for fracture shaft humerus by dynamic compression plating and interlock nailing. AIMS AND OBJECTIVES To compare and study the results of treatment for fracture shaft humerus by dynamic compression plating and interlock nailing in terms of:Radiological union time, Amount of blood loss, Duration of surgery, Functional outcome, Associated radial nerve recovery pattern and Complications such as infection, iatrogenic nerve palsy, delayed union and nonunion.
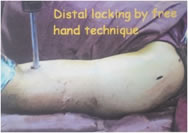
MATERIALS AND METHODS Present study was carried out in the Department of Orthopaedics of Seth Nandalal Dhoot Hospital (Tertiary Care Centre), Aurangabad during August 2004 to August 2006. The study was planned to compare the results of interlock nailing of humerus to a relatively well established technique of dynamic compression plating. Total 44 patients with acute humerus shaft fracture in adults without prior disease were selected retrospectively and prospectively for the study. Twenty-two patients were treated by dynamic compression plating and 22 by interlock nailing. These patients were followed up for a minimum period of 8 months in terms of radiological union time, amount of blood loss, duration of surgery, functional outcome, radial nerve recovery and complications such as infection, iatrogenic nerve palsy and delayed union and non-union. Functional outcome was determined using American Shoulder and Elbow Surgeon's Score. Statistical analysis was performed using students 't' test and 'p' values were determined. Permission from Head of institute was obtained before beginning of the study. Written and informed consent was taken from patient and/or relative. Confidentiality and privacy of data strictly maintained throughout the study period as well as thereafter. Dynamic compression plate manufactured by Sushrut Surgical and Adler Screws were used. Twenty patients were treated by 4.5 mm narrow dynamic compression plate and 2 patients with narrow medullary canal were treated by 3.5 mm dynamic compression plate. Interlocking nails available in diameter of 6, 7 and 8 of Yogeshwar implant were used. 8 mm nail is cannulated and 6,7 mm nails are noncannulated.2.9 mm screw for 6 mm diameter nail and 3.9 mm screws were used for 7and8 mm diameter nails for locking. We used extensive Orthopaedic Trauma Association (OTA) 62 classification of long bone fracture, which includes linear fracture (transverse, oblique, spiral), communited fracture (50%, 50%, butterfly < 50% and > 50%), segmental fractures and fractures with primary bone loss.For open fractures modified Gustilo-Anderson classification (1984)63 used which is based on the size of wound, periosteal soft tissue damage, periosteal stripping and neurovascular injury.
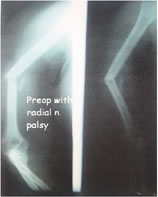
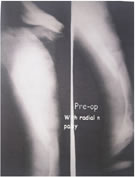
RESULTS The present study consists of 44 cases of acute shaft fracture humerus. All those fractures had specific indications for operation. Care of associated injuries was taken with equal enthusiasm. In polytrauma patient duration of surgery, blood loss was calculated separately for interlock nailing and dynamic compression plating. The data of these cases had been compiled and condensed as a master chart. There was preponderance of male over female (30 Vs. 14) with majority population in 4th decade. The youngest patient was of 26 years and oldest was of 70 years male. Mean age was 39.65 years.In our study, majority of cases were of road traffic accident (86.3%) followed by history of fall from height (11.3%) and only one case of assault. In the present study, out of 44 cases, higher incidence of right-side involvement i.e. 29 patients (65.9%) was observed. Middle third shaft fractures were more common (52.2%) followed by lower and upper third (25%and22.8%) respectively. Transverse fractures were maximum in number (45.4%) followed by oblique (29.6%). There were 6 spiral and 5comminutedfractures.There were 33 (75%) close fractures and 11 (25%) open fractures. In our study, there were 11 open fractures, type II fractures were 7 in number, followed by type III (3 cases) and type I (one case) open fracture. Radial nerve palsy was associated with 2 cases of type II open fractures and one case of type IIIa fracture. There were 12 cases (27.2%) of preoperative radial nerve palsy. Out of 12 cases, 11 had recovered completely. There was no iatrogenic nerve palsy seen in our study. Out of 9 cases explored nerve was found to be intact in 8cases and contused in one case. Most of cases (7) of radial nerve palsy were associated with fracture of middle third shaft humerus. Majority of cases of fracture shaft humerus were associated with head injury followed by lower extremity fracture and ipsilateral forearm bone fracture. Majority of patients (40.9%) were operated within 6hours after injury. Anterolateral approach was used in 16 patients with dynamic compression plating. Posterior approach was used in 6 cases of lower third shaft fracture. Close interlock nailing was performed in 19 patients and open nailing by anterior approach in 3 patients. Majority of fractures in nailing and plating group were united within 17 week (15 V/s 13) respectively. There were 2non-union in plating as compared to one in nailing group. There was highly significant difference between mean values of duration of surgery in nailing and plating group (p<0.01). Thus in dynamic compression plating group the duration of surgery was more than nailing group (58.4 min versus 103.8 min). The average blood loss in plating was 107.2 ml, statistically significant as compared to nailing group (31.5 ml in close and 70 ml in open nailing) (p<0.01). Union rate and time to union were not significantly different in nailing and plating group (14.3 V/s 16.2) (p>0.05). Average radial nerve recovery period was not statistically significant between both groups (9.9 week in nailing and 9.8. week in plating) (p>0.05). At minimum of 8 month follow-up there was no significant difference in functional outcome as per American Shoulder and Elbow Surgeons Score (ASES), strength, range of movement or return to activity in both groups (p>0.05). In the present study, delayed unions were noted in both interlock nail and dynamic compression plating (6 and 7 cases respectively). Complications like infection and iatrogenic radial nerve palsy were not observed in our study. Three cases in nailing group and no case in plating group had impingement, which was statistically significant.
Table 1: Agewise and Genderwise Distribution of Patients
Table 2: Distribution According to Characteristics of Fracture
Table 3: Distribution According to Radial Nerve Injury and Intervention
Table 4: Distribution According to Approach for Surgery of Fracture
Table No 5: Distribution According to Radiological Union Time of Fracture
Table 6: Distribution According to Intra operative and Post-Operative Characteristics of Fracture
DISCUSSION Present study focuses on 44 cases of acute fracture shaft humerus. Twenty-two patients were treated by antegrade interlock nail and 22 were treated by dynamic compression plating and the results were compared with previous series. As per age and sex distribution, 32 patients (73%) were in 3rd and 4th decade, 12 patients (27%) were above 40 years, maximum age being 70 years. These findings were comparable with previous studies19,23 There were 30 male and 14 female patients. Road traffic accident was the most common mode of injury in 86% of cases and males were more commonly involved and the reason for this was that the age group between 20 to 40 years forms the active earning member of the family. Due to early rehabilitation they could return to work early. Transverse fractures were maximum in number (45.4%) followed by oblique (29.6%). There were 6 spiral and 5 comminuted fractures. There were 33 (75%) close fractures and 11 (25%) open fractures. In our study, there were 11 open fractures, type II fractures were 7 in number, followed by type III (3 cases) and type I (one case) open fracture. Out of 12 cases of radial nerve palsy, 3 cases had open fractures, one was treated by debridement, exploration and interlock nail and two were treated by debridement, exploration and dynamic compression plating. In remaining 9 cases who had close injury anatomical reduction was achieved in 3 cases, and were treated by close interlock nail and rest 6 cases in whom reduction was not achieved were treated by exploration and dynamic compression plating. So out of 12 cases nerve was explored in 9 cases. Out of 9 explored, nerve was found to intact in 8 cases and contused in one case. So in majority of cases nerve was intact. Our findings also co-relate with previous studies 16,19 Majority of cases of radial nerve palsy were associated with middle third transverse fractures of shaft followed by oblique and spiral distal third fractures. There were two cases of Holstein and Lewis24 type of fracture, which was treated by exploration of nerve and dynamic compression plating and complete recovery of radial nerve function occurred. There were 9 cases (20%) of head injury followed by fracture lower extremity and fracture forearm bone same side 7cases each which was comparable with study by Chapman et al.23 who showed 17 cases (20%) of head injury in their series of 84 patients. In the present study, 18 patients were operated within 6 hours from the time of injury. Three patients were operated after an interval of 5 to 6 days from the time of injury when they neurologically settled down. There was no significant difference in terms of complications and functional outcome in those who were operated early and late. Average blood loss in interlock nailing (close 31.5 ml, open 70 ml) was significantly less than in plating group (107.2ml) in present study. As plating required extensive surgical dissection, surgery time was significantly more (103.8 min versus 58.4 minutes in nailing group). Lin and Jinn20 in their study of 48 patients reported significantly less blood loss and surgery time in nailing than plating which was comparable to present study. In both groups none of the patient in our study received blood transfusion. There was no significant difference as per functional outcome assessed by American Shoulder and Elbow Surgeon's score and range of movements after minimum 8 months follow-up. This observation was similar to previous series.22,25 In previous reports of dynamic compression plating fixation the incidence of nonunion was ranged from 2 to 10%, of infection 2 to 4% and of iatrogenic radial nerve palsy from 2 to 5%.10,15-17,19 In our dynamic compression plating group there were two nonunion (9%) and infection, iatrogenic nerve palsy was not seen. There was one non-union in interlock nailing group (4%) and no infection and no iatrogenic radial nerve palsy. Impingement occurred in 3 cases of nailing group of which one patient required subacromial Depomedrol injection and symptoms relieved and remaining 2 patients recovered by physiotherapy. In one case of nailing distal screw head broken but it did not interfere with outcome. We did not find shoulder and elbow stiffness in both groups. CONCLUSIONS For patients requiring surgical treatment of humeral shaft fractures, both dynamic compression plating and interlock nailing provide predictable methods for achieving fracture stabilization and ultimate healing. Plating requires extensive dissection, more blood loss and duration of surgery as compared to nailing. Antegrade interlock nailing performed properly is safe, effective and quick method in terms of duration of surgery, amount of blood loss, complications and the method of choice in polytrauma patients. Interlock nailing is more suitable for cases of osteoporotic fractures, comminuted fractures in which plating is not preferable. In cases of fracture shaft humerus with associated radial nerve palsy if anatomical reduction is not possible, exploration of the nerve and fixation is required.
REFERENCES
Policy for Articles with Open Access
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||






 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.