 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 3 Issue 3 - September2017
A randomized controlled trial comparing outcomes of k wire removal at 4 weeks vs. 6 weeks of lateral condyle fractures of humerus in children
Rishabh Kumar1, Santosh Kumar2*, Nishant Kashyap3, Anand Shankar4
1Sr. Resident, 2Professor and HOD, 3Sr. Resident, 4Sr. Resident, Department of Orthopaedics, IGIMS, Patna-800014, Bihar, INDIA. Email: drrishabh2005@gmail.com, drsantoshigimsortho@gmail.com, jhini98@gmail.com, drshanka@gmail.com
Abstract Background and Objectives: Lateral condyle humerus fractures are the most common distal humeral fractures in children. They are associated with higher rate of complications and the results of non-operative management are associated with high rate of later displacement. So a randomised controlled trial comparing outcomes of K-wire removal at four weeks vs. six weeks of lateral condyle fractures of humerus in children was done. Methods: All patients aged one to fourteen years with traumatic fractures of the lateral condyle fracture of humerus presenting to the Department of Orthopaedics, IGIMS giving written consent for the trial were included in the study and randomised in two groups. Fractures more than seven days old were excluded. Cases taken were randomised according to random excel number generation. After open reduction and internal fixation the k-wire removed at four weeks in one group and at six weeks in another group. The clinico-radiological outcomes were evaluated for infection and radiological union. Collected data were evaluated and various statistical tests applied. P-value of less than 0.05 was taken as significant. Results: We found no statistically significant difference in comparison of union or infection with different age groups (p<0.05). Three patients developed skin infection, one in group A and two in group B. All patients did show radiological union at the expected time of k-wire removal two in group A one in group B. Conclusion: Our study has shown that fracture of lateral condyle of humerus united earlier than 6 weeks and shows no significant difference in short term outcome of K-wire and back slab removal at 4 weeks or at 6 weeks regarding union and infection. Key Words: k wire, fracture of humerus.
Fracture of the lateral condyle of the humerus constitutes 10% to 15 % of elbow injuries with the peak occurring at the age of 6-7 years1-8. Pediatric elbow fractures are different from many other pediatric injuries. They are associated with relatively high rate of complications and the results of non operative management are not always good. The child’s elbow is well vascularized and therefore fracture healing takes place very quickly. Such a narrow window of opportunity makes it imperative that the fracture be properly managed very quickly9. The attached extensor muscles displace the fragment from its bed to varying degree. causing displacement which varies from a downward, lateral and usually also backwards with or without rotation of the fragment10. The extent of injury may not be appreciated on x-ray because most of the distal humeral epiphysis is still cartilaginous. In such situations it is helpful to make x-ray of the normal elbow and compare the two sides, paying particular attention to the relationship (alignment) of the long axis of radius, the capitular ossific nucleus and humerus10. Some authors have advised non-operative treatment for closed undispalced fractures and open reduction and K-wire fixation for displaced fractures1,9,11-15. However in later studies by some other authors emphasized the importance of open reduction and K-wire fixation over closed reduction and POP slab application even in undisplaced fractures9,10,16,17-22. They found better results after operative management instead of non-operative management. There is controversy in removal of K-wire at 3-4 weeks or 6 weeks after operative fixation. Few of them remove K-wire at 6 weeks9-12,14,23 and others remove in 3-4 weeks1,2,13,15,24,25. Those who remove the K-wires in 3-4 weeks find that there is less number of infection rates, lesser degree of stiffness and lesser time was required to achieve almost full ROM of elbow joint. Studies have been done in the West which compare the outcomes of removal of K-wires at 3-4 and 6 weeks in the fixation of lateral condyle fracture of humerus in children. The authors have found no significant difference. But the general practice is to remove the K-wires at 6 weeks. If a study here in our setup also shows the same results then we also could remove the K-wires at 4 weeks with the advantage of less infection rates, early mobilization and lesser chance of stiffness.
MATERIALS AND METHODS The study was conducted in the Department of Orthopaedics, IGIMS, a tertiary care hospital in Patna, over a period of twelve months from August 2016 to July 2017. Inclusion Criteria: All patients aged 1 to 14 years with traumatic fractures of the lateral condyle fracture of humerus giving written consent for the trial, fit for anaesthesia, without other distal humeral fracture, without any systemic disease likely to affect the outcome were included in the study. Allocation was randomized using Excel random number generation technique into two groups:- Group A: Removal of K-wire and back slab in 4weeks Group B: Removal of K-wire and back slab in 6 weeks. Following fitness for anesthesia, patients of this group were taken up for surgery and underwent open reduction by lateral approach to elbow and two cross K-wire fixation. Follow Up: After the surgery any immediate post-operative complications were taken into account. They were discharged after 2 days of antibiotics on POP slab, general condition permitting. After discharge all patients were reviewed after 2 weeks for inspection of surgical site whether any infection present or not, if not then sutures were removed. Group A patients were followed up again at 4 weeks for radiological union, signs of infection, K-wire and back slab removal and physiotherapy. At 6 weeks group B patients were followed up for radiological union, signs of infection, K-wire and back slab removal and physiotherapy. Group A patients were again followed up at 6 weeks to observe any deformity. At 12weeks both groups were followed to observe any deformity. Statistical Analysis: A student ‘t’ test and 95 % confidence intervals were used to evaluate the difference between the two treatment groups with respect to numerical variables including age, time from injury to hospital. Table A1: Correlation between age gr. and study gr.
Our study shows that most of the patients are male in both the study groups. There is no significant correlation between age and sex with study group showing success of randomization.
Table B1: Comparison of mode of injury with study gr.
Our study shows that Milch type II fracture is much more common than Milch type I in both the study groups.
TableB2: Comparison between type of # and age gr.
Table B3: Comparison of injury to hospital time
Table C1: Comparison of infection at 2 weeks with study group
Table C2: Comparison of infection at the time of K-wire removal with study group
Table D1: Comparison of Union with study group
Table D2: Comparison of type of fracture with union
Table D3: Comparison of union in different age groups
There was no intra-op and immediate post-op complication noted. At the end of 12 weeks of follow up, there was no deformity seen in any case, all cases regained almost comparable range of motion with normal side.
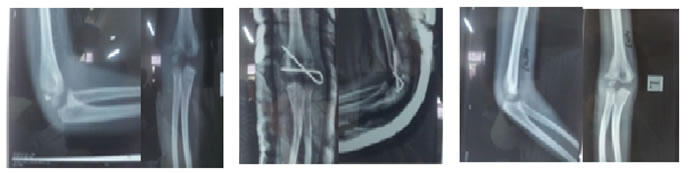
Figure 1: (Radiographic picture) A: Pre op showing Fracture (B): Showing post-op pic (C): Showing 6 wks post-op (after K-wire removal)
Figure 2: (Radiographic picture) G: Pre op showing Fracture (H): Showing immediate post-op radiograph (I): Showing 4wks post-op showing signs of union.
DISCUSSION Our study shows the mean age of incidence to be 7.05 ± 2.78 years. Our study shows that about 14 % of cases of elbow injuries in children is showing lateral condyle fracture of humerus. Most of the patients were male in our study. In one study all the patients were male.7 About 37 percent of the total patients had injury by fall from 4-6 feet height which highly corroborates with the mode of injury by fall from monkey bars (usual height is 4-6 feet) in a study.26 In contrast to this finding one study shows that fall from height (bicycle 33 percent, tree 16 percent and monkey bar 16 percent) is more common mode of injury.13 Milch type II fracture was more common than Milch type I fracture in total patients in my study. Involvement of left side (number of cases 41) of humerus is more than the right side (number of cases 29) out of total seventy cases in our study. This finding has also been described in other studies.7,15,17,27 In our study out of seventy cases more than half of the patients (37 patients 52.86 percent) reached within 24 hours of injury and were treated on the same day on emergency basis. Rest of the patients reached to hospital after 24 hours but operated within 7 days. Those patients who came after 7 days of injury were excluded from the study. In one of the studies 25 patients (24percent) were treated on same day of injury, 62 patients (60 percent) were treated next day, Between 2-7 days 12 patients (11 percent) were treated and only 5 patients (about 5 percent) were treated within 8-17 days of injury.26 One of the studies excluded all the patients who underwent operative fixation after 14 days.28 In contrast to these studies one study treated 12 patients between 1-4 weeks, 5 patients between 5-8 weeks and 5 patients between 9-12 weeks.24 There are other studies in which fixation of fracture has been done after 3 weeks of injury.7,29 Comparison of infection has been done in different study groups at the time of suture removal and at the time of K-wire removal. It has been found that only one patient in study group A and 3 cases in study group B shows signs of superficial infection at the time of suture removal i.e. 2 weeks. These cases were successfully treated with wound dressing and intravenous antibiotics successfully. One of the previous studies in which K-wire and back slab was removed in 3-4 weeks as our group A had one case of superficial infection which resolved with antibiotics.26 Other studies in which K-wires and back slab/cast was removed at 3-4 weeks found no infection in their patients.13,27 One of the studies who removed K-wire and back slab at 6 weeks as our group B found three cases of pin tract infection which were treated successfully by oral antibiotics.24 Other studies who removed K-wire and back slab/cast at or after 6 weeks had no cases of infection.15,28 In our study there were only one cases in study group A which did not show radiological union at 4 weeks but on further follow up both cases had radiological union at 6thweek. There was one case which does not had radiological union at 3rd week in one of the previous studies as our group A. K-wire reinserted for 2 more weeks but still there was no radiological union. Finally fracture united after fixation with cannulated screw across the metaphyseal fragment of the lateral condyle into the distal metaphysis of the humerus.26 There was only one case which did not show radiological union in study group B at the end of sixth week, on further follow up at 12th week the fracture was radiologically united. All of the cases had radiological union at the end of six weeks in other studies.15,28 In contrast to above studies the average time period of radiological union in one of the previous studies was 8 weeks.24 Our study clearly shows that all the cases that does not had radiological union at the time of K-wire removal according to their respective study group belongs to age group of greater than 10 years. No study was found comparing these two parameters.
CONCLUSION Our study has shown that fracture of lateral condyle of humerus united earlier than 6 weeks and shows no significant difference in short term outcome of K-wire and back slab removal at 4 weeks or at 6 weeks regarding union and infection. Further evaluation of short term as well as long term outcome is needed with more number of cases in various aspects.
REFERENCES
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.