 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 4 Issue 1 - October 2017
Approach to hand infections: Our experience
Pendyala Sugnaneshwar1, Sambandhamurthy Venkat Raman2*
1Assistant Professor, 2Associate Professor, Department of Orthopaedics, Kamineni Institute of Medical Sciences, Sreepuram, Narketpally, Nalgonda District, Telangana, INDIA. Email: drvraman@gmail.com
Abstract Objectives: To study clinical incidence, aetiology, and outcome of hand infections. Materials and Methods: This is a prospective study and analysis of hand infections in about 90 cases. Detailed history, of mode of trauma, swabs for wound culture, and sensitivity, and radiographs were done for all these cases. Injection Tetanus toxoid, was routinely provided Simple cases were managed as day care. Conclusion: Our study indicates, that stressing on the need for public health awareness and education, early recognition of all hand injuries even trivial ones, and a proactive vigorous, prompt treatment of every case of hand trauma, to avoid, loss of man hours, and prevent morbidity in each individual. Key Words: Injury, hand infection, prompt treatment.
The hand is the greatest asset in man, and productivity, and myriad daily activities of a man depend upon a normal, sensitive, pliant, healthy hand. Stereognisis, and expression of our feelings depend upon our hands, and in fact, a hand is one of the most prized possessions of mankind. Even today, in this modern world, much of our productivity is done directly by hands, or through machinery, and tools which is in turn operated by hand.1 Thus hand injury, is a reasonably common occurrence, in everyday life, and such injuries are bound to get infected, if not treated promptly, and diligently. Even trivial injuries can have disastrous complications, if not anticipated, and treated in time as some of the most virulent microorganisms, can travel, into the lymphatics, and synovium2, even through tiny punctures, or thorn pricks 2 Fatalities were common, before the discovery of antibiotics, causing loss to life and limb. With the discovery of antibiotics, and anaesthetic agents, and also refined surgical techniques, the outcome nowadays, is much more improved. And total, or partial amputations have become a rarity3. First aid facilities, public health awareness, and education, and mandatory availability of Employees State Health Insurance schemes have contributed enormously to avoiding/treating these complications Modern developments in microsurgical techniques and physiotherapy, and rehabilitative medicine, have developed tremendously, helping hand surgeons reimplant, amputated digits/hands. This has caused a separate subspeciality called Hand surgery.4
MATERIALS AND METHOD A total of 100 patients of hand infections were managed between the period of March 2003 and June 2005, at Mediciti Institute of Medical Sciences (MIMS), Ghanpur, Medchal Mandal, Ranga Reddy District, Andhra Pradesh. All hand infections, irrespective of their aetiology were included in our study. All patients, after informed consent, were examined thoroughly for distal neurovascular deficiencies, after taking complete history, blood investigations, which included haemoglobin, Erythrocyte Sedimentation Rate, Total WBC count, differential count, bleeding time, clotting time, HIV, HBs Ag, complete urine examination, random blood glucose level, s blood urea, serum creatinine, was done. A plain radiograph of the hand antero-posterior, and oblique view was taken. A swab of the injured site was taken for a culture and sensitivity analysis. An intravenous broadspectrum antibiotic was routinely started, pending culture sensitivity report. All hands were splinted in functional position, and elevation, and active finger movements were encouraged from day one. After complete healing, as assessed clinically, these patients were subjected to follow up, on a weekly basis, for a month, and then once in 15 days, for three months, and active, physiotherapy was encouraged.
RESULTS
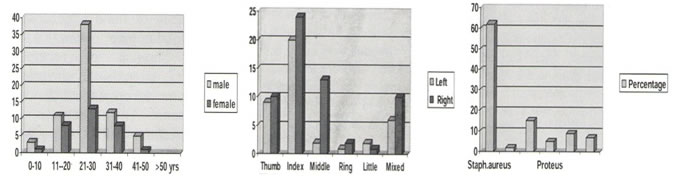
Figure 1: Distribution of cases with respect to age and sex Figure 2: Distribution of cases with respect to site of infection Figure 3: Distribution of cases with respect to organism
COMPLICATIONS In our series, 06 patients, were lost to follow up, and of the remaining 94, the most common complications were stiffness of the fingers, and loss of sensitivity, which recovered to some extent. Stiffness of hand was relieved, with further vigorous physiotherapy.
DISCUSSION Although hand infections, can result in severe disability, due to stiffness, and contribute significantly, to lost man hours, awareness, of the potential hazards of neglecting, such infections, or not treating them proactively, and diligently, has to be stressed. after proper, counselling of these patients. Farm sector, with the attendant danger of tetanus, and industrial accidents, involving machinery, still continues to contribute, significantly to these group of injuries.5. Women, and children, constituted a minor portion of these patients, the bulk majority being men, and the dominant hand being most often involved. Manual, farm labourers,6-10, and employees with industrial accidents, were often the victims, while road traffic accidents, contributed to a small percentage. More than 80% of these hand injuries/infections, were observed in men in their 30 s, and 40 s., i.e. in men in the prime of their lives. Such workers were often the sole bread winners in their families, and it was imperative that they return to their work at the earliest. Earlier literature reveals that the commonest site of infection was in the pulp space, but now, in the past decade, deep palmar infections, are showing a recrudescence. Growing resistance to staphylococcal, and pseudomonas, is rearing its ugly head. A good number of our cases needed surgical intervention, in the form of minimal debridement11. With our approach, there has been a marked decline in the morbidity of hand infections, by way of decline in lost man hours, sickness absenteeism, and much less incidence of amputations and an early return to their work. We have stressed on the importance of awareness, counseling, proactive treatment, even for trivial injuries.
CONCLUSION Our series, stresses on the need for public health education, early recognition of possible complications, even in trivial injuries, and prompt, treatment, in each and every case.12.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.