 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 4 Issue 2 - November 2017
Analysis of functional and radiological outcomes in hybrid total hip replacement
Bharath1, Vishnu Vijayaraghavan2, Thirunthaiyan3, R Doraikumar4*
Department of Orthopaedics, Sri Ramachandra University, Porur, Chennai, INDIA. Email: bharathsek23@gmail.com
Abstract Background: Arthroplasty is being widely used nowadays to restore the function of the hip following various conditions affecting the hip. The concept of replacing the head with an artificial head and socket thereby replacing the joint, had a profound impact on the treatment of painful hips especially associated with a degenerative process. Hybrid total hip replacement came about to minimise the complications that were associated with cemented and un-cemented total hip replacement. Materials and Method: Twenty two total hip replacements were carried out in 22 patients in the period from 2015 to 2017. All the patients were assessed functional and radiologically with a period 1-2 years using Harris hip score. All patients were operated through Moore southern approach. All these patients were assessed pre operatively and post operatively with the Harris hip score and radiograph in anteroposterior and lateral projections. Results: The age of patients at the time of surgery was years. Indications for the operation included avascular necrosis in 6, rheumatoid arthritis in 1, ankylosing spondylitis in 3, inter-trochanteric fracture in 3 and fracture neck of femur in 9 patients. The results evaluated according to the Harris classification system were excellent or very good in 84.23.%, satisfactory in 18 % and poor in 0% of the replacements. On subjective evaluation,4 patients presented with groin pain (18.18%). Aseptic loosening was developed in 4.5% and dislocation 4.5%. Conclusions: Harris Hip score was found to be relatively equal in all patients with Hybrid Total Hip Replacement showing 84% of excellent/good results in our series. It leads us to believe that un-cemented acetabular cup with a cemented femoral stem is likely to last longer. Key Word: Hybrid total hip arthroplasty, Harris hip score.
The hip joint connects the lower limbs and the pelvis. It has been specifically designed for stability as well as to accommodate a wide range of movements. Being a multi-axial ball and socket joint, it allows the entire lower limb to move in three planes of motion. It also functions as a shock absorber for the trunk and upper body. The most important cause for restriction of human movement is pain in the hip joint. The causes of this pain can vary from various causes such as fracture neck of femur in elderly patients to ankylosing spondylitis at a younger age. Arthroplasty is one common procedure that is being primarily used to restore the stability and motion of the affected hip. The concept of replacing the degenerated head with an artificial head and socket thereby replacing the joint, had a profound impact on the treatment of painful hips especially associated with a degenerative process. Hybrid total hip replacement came about to minimise the complications that were associated with cemented and un-cemented total hip replacement. Examples of these complications were aseptic loosening of acetabular components in cemented total hip arthroplasty. Cemented total hip arthroplasty techniques improved and were used in younger patients as well for a time. But, failures of cement-less femoral stem fixation are on account of little bone growth, thigh pain and subsidence of femoral component. Along with this, favourable results were reported with respect to cement-less acetabular components. Hence the concept of hybrid total hip replacement came about, using a cement-less acetabular component and a cemented femoral component. This study was carried out to assess the outcomes following hybrid total hip arthroplasty following various condition affecting the hip.
MATERIALS AND METHOD Twenty two total hip replacements were carried out in 22 patients in the period from 2015 to 2017. All the patients were assessed functional and radiologically with a period 1-2 years using Harris hip score. All the patients were operated through Moore’s southern approach. All these patients were assessed pre operatively and post operatively with the Harris hip score and radiographs in anteroposterior and lateral projections. Preoperative planning also include the use of plastic overlap templates supplied by the prosthesis manufacturers. Templating aids in selection of the type of implant which will provide the best fit implant size and neck length required to restore equal limb length and medical offset.
RESULTS Mean Harris Hip Score Table 1: Conditionpre oplatest
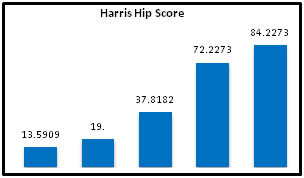
The mean Pre op HHS in this study was 13.59 and the latest HHS was– 84.2 at the follow up in 15 months
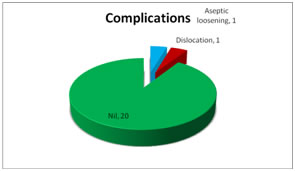
Figure 1: Mean HHS in follow ups Out of 22 patients 18 patients were found to have excellent/good results. Four patients had fair results. One case of femoral loosening at follow up of 6 months. Patient underwent revision total hip arthroplasty. 17 patients with neutral (77%) 2 were with vertical 9% and 3 with horizontal (13) acetabular cup placement. Femoral stem were placed neutral in 15 patients 68%, valgus in 7 patients32%. We had one case of dislocation in our study Complications Figure 2: Figure 3: DISCUSSION The following parameters includes Pain, Limp, Support, Walking distance, Stair climbing, Range of movements, Limb length discrepancy, were used in evaluation and comparison of clinical outcome in our study. Four patients had presented with groin pain (18.18%) which is compared with the Carlinsoui AS, Gentz and Linder L 14%, Thomas P. Schmalzried, William. H. Harris 18%30. In all the patients the pain was predominantly over the groin region and was not a radiating type of pain. No patient had anterior thigh pain which is usually associated with un-cemented femoral stems. The pain was a dull, aching, non radiating type of pain which resolved over time in the postoperative period and did not cause any interference in post operative rehabilitation or activity. No patient had a marked limp on the side that the patient was operated on. 20 patients did not use any support to walk after 3 months. Two patients walked with support due to their elderly status and general weak constitution. Out of 22 patients, 19 patients were able to walk for long distances. Two patients were unable to do due to their age and general constitution and were only able to walk for half a kilometre, and one patient with AVN is not able to due to pain in the opposite hip. At the latest post operative review, 13 patients are able to climb stairs without the assistance of the rail, 5 patients could climb stairs with the assistance of the side rail, and 4 patients are able to climb the stairs with difficulty. After assessment of the functional outcome post operatively, 20 patients had a good range of movement with range of movements reaching up to 80%. Two patients had only a relatively less range of movements within the range of fair. No patients after assessment were found to have poor range of movements. In our study 3 patients (13.63%) had shortening of approximately 1cm. Foot wear correction was given for these patients Other studies similar to this one have also reported the statistics of limb length discrepancy that they have encountered during their study Jasty M, Webster W and Harris W reported 16% limb length discrepancy in a total of 85 total hip replacements using a parameter of shortening of 1cm15. Even today limb length discrepancy is a major problem encountered during total hip arthroplasty’s. Careful measuring, assessment and pre operative planning are required in order to hopefully avoid these complications. In a case of limb length inequality it is always imperative to evaluate the patient clinically and radiologically in order to identify any underlying condition or complication that may be the cause of the limb length discrepancy. The mean Pre op Harris Hip score in our study is 13.59 and latest Harris hip score is 84.23. This can be compared to the study by Wixson et al whose mean pre op and post op Harris hip score were 44 and 93 respectively. (JBJS Vol 73 feb ’91) MEAN HHS STUDY PRE OP HHS LATEST HHS OURS 13.59 84.23 WIXSON ET AL 44 93 SIWACH ET AL29 44 83.5 CLOHISY ET AL34 48 92 After the patients underwent Hybrid total hip arthroplasty there was remarkable improvement as has been shown by our analysis of the harris hip score over the period of our study. The greatest change in the Harris hip score occurred between our assessment at the pre operative point and at their assessment at review at 6 months. For most of our patients our study extends till review at 12 months and most of our patients had a steady improvement in Harris Hip score till date. For each of the conditions that we treated using Hybrid Total Hip Arthroplasty Inter-trochanteric fractures had a remarkably good result followed by Neck of femur fractures followed by Avascular necrosis. Rheumatoid arthritis patient had a lower HHS at latest review than others due to multiple joint involvement. In our case series treated with Hybrid Total Hip Replacement, after a short follow up we have 0% excellent results, 82% good results, and 18% fair results and no poor result which is comparable with Thomas P. Schmalzried who had 91% excellent to good results in a 6.5 year follow up study of the same (JBJS VOL.75-B No.4 July 1993).
CONCLUSION In this study, a short term follow up of Hybrid Total Hip Replacement has been attempted and found 82% of excellent/good results. We also found that the results in patients in Inter-trochanteric fractures and fractures of the neck of the femur and Avascular Necrosis were better than those of the patients with Ankylosing Spondylitis and Rheumatoid Arthritis. But by analysis, the progressive increase in the Harris Hip Score was found to be relatively equal in all the patients. Symptoms like anterior thigh pain which are usually associated with un-cemented femoral stems were not experienced by any of the patients. From a financial perspective, the cost of the cemented femoral stem is relatively less. An un-cemented acetabular cup with a cemented femoral stem is likely to last longer than a cemented one. But ours is a short term follow up and this will require more study.
REFERENCES
|
|

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.