 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 4 Issue 3 - December 2017
Serum calcium level – A sensitive predictor of risk of fragile hip fracture in elderly Indian population
Gadde Saikrishna1, V Ramnarayan2*, M Mohan Kumar3
1Resident, 2Associate Professor, 3Professor, Department of Orthopaedics, Sri Ramachandra University, Chennai–600116, Tamil Nadu, INDIA.
Abstract Background: Skeletal system is considered to be the internal construct of the human body and Calcium is the major component of it. Calcium exists as insoluble inorganic salts with phosphorous in the bone, aiding the mineralisation of the osteoid matrix thereby imparting strength and resistance to stress and deforming forces. Extra skeletal calcium gets circulated in the body performing multiple physological activities. Human physiology has always given prime importance to these vital functions and maintains a near constant serum calcium levels within a narrow range. Any change in this level is discussed to cause resorption of the bone primarily and release the calcium stores, making it weak and elastic which makes them susceptible to fragile fractures. This study focuses on the predictive value of serum calcium to identify the risk of fragile hip fracture. Aim of the study: To estimate the serum calcium levels in elderly patients with hip fractures and compare them with that of the age matched control subjects and evaluate the relation between serum calcium level and fragile hip fractures. Materials and Methods: This is a prospective, case-control study conducted at Sri Ramachandra University, Chennai between July 2015 and July 2017. All the patients in the study are older than 65 years. The total sample of the study is 200 individuals (male - 73; female - 127) of which 100 patients (male – 37; female – 63 ) are with fragile hip fractures (neck of femur and Intertrochanteric) form the cases group and the other 100 patients form the control group ( male – 36 ; female – 64 ) who are age matched individuals without fragile hip fractures at the time of assessment. Patients younger than 65 years, with history of prior calcium supplementation, chronic steroid users, anti epileptic and anti malignant drug users, with history of chronic liver and kidney failure, malabsorption syndrome are excluded. Serum calcium is estimated from the individuals of both the groups and subjected to statistical analysis. Results: The mean value of serum calcium of the total sample is 8.995mg/d; (0.7670 S.D). The mean values of serum calcium in the case and control groups are 8.777mg/dl (0.7384 S.D) and 9.213mg/dl (0.7358 S.D) respectively. The mean serum calcium level is comparatively lesser in the patients with fragile hip fractures. There is a statistically significant difference between the serum calcium levels of both the groups (p=0.000). Conclusion: Low serum calcium level has a direct relation with the increased chance of developing a fragile hip fracture in elderly population. Serum Calcium may be considered as a sensitive predictor of the risk of a fragile hip fracture. Key Words: Serum Calcium, fragile hip fractures.
Skeletal strength is majorly dependant on the inorganic matrix formed by the product of calcium and phosphorous, making the bone resistant to high degree of stress. Bone acts as a major reserve (99%) of calcium in the body. The rest is distributed in the Extra and Intra cellular fluids contributing to the extraskeletal vital functions of the body like blood coagulation cascade, neural excitability, voluntary and involuntary muscles contraction which cannot be compromised. Thereby making this minor extraskeletal part of calcium a prime regulator of calcium homeostasis in the human body. The normal serum calcium range has to be maintained within a narrow range of 8.8 to 10.8mg/dl for smooth processing of the above mentioned programs. Alteration of serum calcium level is immediately put back to the normal in a healthy individual by Parathyroid hormone, Calcitonin and Vitamin D which are activated by their respective feedback mechanisms. Hypocalcemia stimulates the parafollicular cells of parathyroid glands to secrete parathyroid hormone (PTH), whose major function is to maintain the serum calcium level within the physiologically acceptable range by various mechanisms among which calcium resorption from the bone is the primary one. Sequential resoprtion of bony calcium and increased phosphate excretion through kidneys by PTH makes the bone devoid of its mineral component and left out with the osteoid matrix which do not have adequate strength to bear the stress and turn fragile. Hip fractures due to trivial and domestic injuries are very common among elderly population associated with long durations of immobilisation increasing the morbidity of the individual with the incident of complications like respiratory infections, thrombotic sequale, skin necrosis, faulty dietary practices and electrolyte imbalances. The treatment and recovery also depends on the bone stock of the fracture site, whereas elderly patients do fall in the claws of Osteomalacia and Osteoporosis making the situation complicated. Bone resorption mainly occurs in the weight bearing cancellous and cortico-cancellous weight bearing zone of the skeleton making it even more susceptible to fragile fractures due to a minor violence. This study mainly concentrates on the relation of serum calcium and hip fractures and also the predictive value of serum calcium in identifying the risk of sustaining a hip fracture in elderly population due to trivial trauma.
MATERIALS AND METHODS We conducted a prospective, case-control study at Sri Ramachandra University, a tertiary care hospital in Chennai between July 2015 and July 2017. A total sample of 200 individuals (n=200) who are older than 65 years are considered in this study of which 73 are male and 127 are female. In the case group of 100 patients (n=100), individuals with fragile hip fractures are considered of which 37 are male and 63 are female. In the control group of 100 patients (n=100), age matched individuals without a fragile hip fracture are considered of which 36 are male and 64 are female. Individuals with history of high velocity injuries, age less than 65 years, history of prior calcium supplementation, chronic streroid, anti epileptic and anti malignant drug usage, individuals with malabsorption syndromes, chronic liver and renal disease are excluded from the study. After obtaining an informed consent from the participants of the study, using sterile phlebotomy techniques, blood samples are withdrawn and serum calcium level is measured using O-Cresophthalein Complexone technique and 8.8-10.8mg/dl is considered as the normal range of serum calcium. Fracture radiology is assessed on the plain radiographs of the pelvis with both hips to evaluate the pattern of fracture i.e. either neck of femur fracture or Intertrochanteric fracture. The type of neck of femur fracture is decided using Garden classification and type of Intertrochanteric fracture using Boyd and Griffin classification. The collected data were analysed with IBM.SPSS statistics software 23.0 Version. To describe about the data descriptive statistics frequency analysis, percentage analysis were used for categorical variables and the mean and S.D were used for continuous variables. To find the significant difference between the bivariate samples in Independent groups the Unpaired samples t-test was used. For the multivariate analysis the Kruskal Walli's test was used. To assess the relationship between the variables Spearman's rank Correlation was used. To find the significance in categorical data Chi-Square test was used. In all the above statistical tools the probability value 0.05 is considered as significant level. Once we got the results, we compared the serum calcium levels of both cases and control groups and checked if it had any statistical significance.
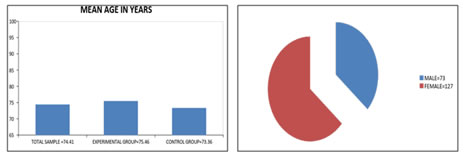
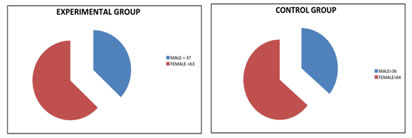
RESULTS If we observe the demographics of the study, the mean age of the total sample of 200 patients is 74.41years (6.983 S.D) and the mean ages of case and control groups are 75.46years (7.449 S.D) and 73.36 years (6.348 S.D) respectively. The male and female population in the total study sample are 73 and 127 respectively. No significant bias is noted due to gender distribution which shall affect the final study result (p = 0.883). Similarly the male and female population in the cases and control groups are 37,63 and 36,64 respectively with no significant difference in the gender distribution among both the study groups.
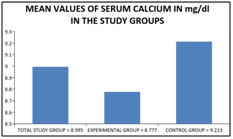
Figure 1: Figure 2: Figure 3: Figure 4: Figure 5: Legend Figure 1: Mean age in years of the population in all the study groups; Figure 2: Gender distribution in total study sample; Figure 3: Gender distribution in the cases group; Figure 4: Gender distribution in the control group; Figure 5: Serum calcium status in the study groups Table 1:
Also when the frequency of falls sustained by the individuals is considered; in the total study sample of 200 patients, the mean frequency of falls in the past one year is 1.00 times (0.967S.D). In the cases group, the mean frequency of falls in the past one year is 1.65 times (0.883 S.D). In the control group of 100 patients, the mean frequency of falls in the past one year is 0.35 times (0.575 S.D). A statistically significant difference is noted in the number of falls sustained by the individuals between the cases and control groups.
Table 2:
DISCUSSION Metabolic bone disease; either Osteoporosis or Osteomalacia is often discussed to be the contributing factor for weakening of bone and increased risk of devastating fractures especially in hip and spine even with a trivial injury in elderly population of developing countries, increasing their mortality and morbidity. Currently our study mainly concentrates on serum calcium levels estimation and to evaluate its relation with hip fracture and its role in predicting the risk of sustaining a hip fracture in elderly Indian population. Low serum calcium mobilises calcium reserves from the bone and cause profound Osteomalacia due to secondary hyperparathyroidism, hence the importance of maintaining a physiologically acceptable range is mandatory. Therefore the concept of linking lower serum calcium levels to the increased risk of hip fracture appear to be sensible, whereas considering this to be a sensitive parameter in predicting the risk of developing a hip fracture has not been proved universally. Differences in the assay and sample test methods, subject populations and analytic platforms used in the studies may explain the inconsistencies among the studies. In this prospective case-control study we estimated the serum calcium levels in the cases group which comprise of elderly patients with hip fractures and in the control group which comprise of age matched healthy individuals and we have noticed a statistically significant (p=0.000) low mean serum calcium level in the cases group population i.e. 8.777mg/dl (0.7384 S.D) when compared to that in the control group population i.e. 9.213mg/dl (0.7358 S.D). Thereby serum calcium arises as an important biochemical marker in estimating or predicting the risk of sustaining a hip fracture in elderly population. Similar to our result, Gau et al1 when conducted a case-control study have suggested that lower serum calcium levels are significantly associated with higher risk of hip fracture and Formosa et al2 also concluded that serum calcium level could be indicative of fracture risk. Whereas, C. Cooper et al3 when conducted a similar study found that the serum calcium levels in both cases and control groups appeared to be similar with no significant difference. Fishbane et al4 though conducted a similar study, it is done in patients undergoing haemodialysis and serum calcium is declared to be associated with higher risk of hip fractures. This study also identified that there is statistically significant increased frequency of falls in the cases group population when compared to that of the control group. This may be related to the low serum calcium levels in the cases group population and can be explained by the increased proximal group of muscle weakness due to hypocalcemia, thereby decreasing the balance and making the individual more susceptible to have a fall and sustain a hip fracture. Hardly any study has been done to evaluate the direct association between low serum calcium levels and the risk of fall. Mastaglia SR et al5, Cedric Annweiler et al6, Sakuma et al7 concluded that Hypovitaminosis D is associated with increased risk of fall which indirectly targets at the role of Hypocalcemia in increased risk of falls. Our study do have limitations, as the immediate changes in the serum calcium levels or metabolism occurring after sustaining a hip fracture are not considered. The risk of fall in elderly population can be related to the multiple other factors like usage of sedatives, impaired vision and cognitive impairment which are not taken into account in our current study.
CONCLUSION We thereby conclude that Serum Calcium can be considered as a sensitive parameter in predicting the risk of sustaining a hip fracture. Hypocalcemia is directly associated with the increased risk of hip fracture in elderly Indian population and may be related with the increased frequency of falls.
REFERENCES
|
|
|||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.