 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 4 Issue 3 - December 2017
Functional outcome of proximal femoral plating in unstable trochanteric and sub-trochanteric fractures
K Balagopal1, Jose George2*, Jose Francis C3
1Additional Professor, 2Sr. Resident, 3Professor and HOD, Department of Orthopedics, Government Medical College, Thrissur, INDIA. Email: kbalagopal1201@gmail.com
Abstract The occurrence of proximal Femoral fractures in our elderly population is increasing with rise in life expectancy. Newer implants and advanced techniques for treating such fractures elevate the level confidence of the Surgeon. Proximal Femoral locking plate is one of the newer introductions to the Orthopedic armamentarium. This prospective observational study reports the functional outcome of treatment with PFP. 26 patients with either unstable inter trochanteric fracture or sub trochanteric fracture fitting for the inclusion criteria who came to Orthopedic Department of Thrissur medical college between 1/1/2015 and 1/1/2016 were surgically treated with open reduction and internal fixation with PFP. Muscle strengthening and range of motion exercises were started in the immediate postoperative period. They were followed up clinically and radiologically for six months. Functional outcome was assessed after 6 months using Harris Hip score. Key Words: Proximal Femoral Plate; Unstable trochanteric fracture; Functional outcome.
Peri-trochanteric fractures are one of the most common injuries of old age that necessitate hospital admission and surgical treatment.These fractures are commonly caused by trivial trauma except in young adults. Gulberg1 has proposed that the total number of proximal femoral fractures worldwide will reach 2.6 million by 2025. Hagino et al reported that the whole lifetime risk of Proximal Femoral fracture for individuals at 50 years of age is 5.6% for men and 20.0% for ladies2. Any co morbid condition associated with bone loss, like Diabetes Mellitus, Hyperparathyroidism, Hyperthyroidism and Cushing’s syndrome is associated with an elevation in the risk for hip fracture3. The management of these fractures are always a challenging problem for the treating orthopedic surgeons because of associated co-morbidities, fracture comminution, poor bone quality and difficulty in selecting the optimum implant for fixation. Some of these fractures are highly unstable and hence most of the time fixation is inadequate and hence likely to fail. Unstable trochanteric fractures are trochanteric fractures with large lesser trochanteric fragment, sub-trochanteric extension, comminuted posteromedial cortex, lateral wall deficiency, reverse oblique fractures, and extension to the femoral neck. It is better to treat these fractures surgically as the non-operative treatment often fails. Various devices are available for the fixation of these fractures. Extra medullary devices such as Dynamic Hip Screws, Proximal Femoral Plating, Mc Laughlin's plate and screws, Medoff’s plate and screws, Contoured broad DCP, newer A- O plates, and Intra medullary devices like Gamma nails, PFN, Ender nail, Zickel nail are used to fix the proximal femoral fractures. There are a lot of newer developments that have occurred in this field such as advanced techniques of fixation, modification and improvisation of implants, and various closed procedures. One among those is Proximal femoral locking plate, which can provide a stress shield for the lateral trochanteric wall and prevent lateral migration of proximal fragments. This kind of implant may be a good choice for sub trochanteric or unstable intertrochanteric fractures. Clinical and functional results of PFP is widely accepted and well proven by different studies4 As proximal femoral plating is a newer method which gained popularity in a short period of time, it is worth to study the functional outcome of this method in our scenario. Even though neck of Femur fractures, isolated greater trochanteric fractures and stable intertrochanteric fractures come under the peritrochanteric fractures, they were not included in the present study.Here I report the outcome of PFLP for the treatment of unstable Intertrochantric and Subtrochanteric femoral fractures using open technique.
MATERIAL AND METHODS Patients were admitted from the OPD or Emergency Department. Limb will be supported by upper Tibial skeletal traction with a Bohler Braun splint before surgery. Pre-operative work up was completed and an informed written consent was obtained. Fractures were classified according to the AO Foundation/Orthopaedic Trauma Association classification, and type 31A1 are excluded. Pre anesthesia checkups were completed prior to the day of surgery. Operative Management: After attaining adequate anesthesia, patient was positioned supine with traction on a fracture table. Fracture was reduced under fluoroscopic guidance by closed manipulation and traction. AP and lateral image were obtained and saved for reference. Standard methods of scrubbing, painting and draping were followed. Watson-Jones approach to proximal femur was followed. Fascia lata was split along the skin incision. Vastuslateralis was released from its origin leaving a cuff of tissue proximally for reattachment after fracture fixation. Fracture was reduced and alignment was checked under fluoroscopy. Rotation alignment of limb was also corrected. Proximal femoral locking plate was introduced through the proximal part of incision. A long plate was used to reduce the screw density. Temporary fixation was doneproximally and distally. A cortical screw may be used for reducing shaft to the plate which can be changed to locking screw later. Proximal locking screws were put under fluoroscopic control without altering the alignment. Unicortial screw was used in distal most hole. As many as locking screws were put in proximal segment. At least 4 cortical locking screws were put in distal segment. Primary autogenous bone grafting were done in cases with severe bone loss. After hemostasis, and washing with sterile normal saline, drain was fixed. Vastuslateralis origin re attached. Fascia closed. Skin closed in layers. Dressings given. Length of incision, amount of blood lose, operation time and intraoperative findings were recorded. Post Operative Management: Adequate analgesics were provided. IV third generation Cephalosporin were administered post operatively up to day 7. Dressings were changed on post op day 3, 6and staples were removed by post op day 10. Upper body mobilization was started on post op day 2. Isometric quadriceps exercises were started on post op day 3. Sutures were removed and patients were discharged on post op day 10. When the pain subsided, patients were advised to start non-weight bearing hip range of movement exercises. Follow Up: Patients were followed up regularly after 2 weeks, 1month, 2months, 3 months, 4 months, 5 months and 6 months of discharge. AP and lateral plane X-ray radiograph of proximal femur with hip was taken and radiological signs of fracture union were assessed. If the fracture showed the onset of radiological union, the patient was allowed for partial weight bearing with a square frame walker support. After obtaining radiological union patients were advised to walk without support. Details of each visit were recorded in the Performa of each patient. Evaluation of Functional Outcome: Functional outcome is evaluated using Harris Hip Score5 after 6 months of surgery during the follow up visit.
OBSERVATIONS AND RESULTS Functional outcome of 26 cases of peritrochanteric fractures fixed with proximal femoral locking plate were analyzed and following results were obtained. Age Distrebution: Peritrochanteric fractures can occur at any age but it is quite rare below 45 years of age. In our series the range of age was between 33 and 85years and the mean age is 67.80years. The incidence was highest in the age group of 65 – 85 years. Sex Distribution: Among 26 cases, 16 cases (62 %) were males and 10 cases (38%) were females. Mode of Injury: Among the 26 cases, 23 (88%) fractures were sustained as a result of fall whereas 3 (12%) fractures were due to RTA. Type of Fracture: Off the 26 cases, 15 (58%) were intertrochanteric and 11 (42%) were sub trochanteric fractures. Duration of Hospital Stay: The average duration of stay in the hospital was 21.5days. All the patients were discharged on postoperative day 10 after suture removal. Operation Time: Average operation time was 88.5, which ranges from 70 minutes to 120 minutes, excluding the time for anesthesia and draping. Average Blood Loss: Average blood loss in the study was 300 ml which ranges from 150 ml to 450 ml. post-operative transfusion was given for 14 out of 26 cases and intra operative transfusion was given for 3 out of 26 patients.
Table 1: Post Operative Complications
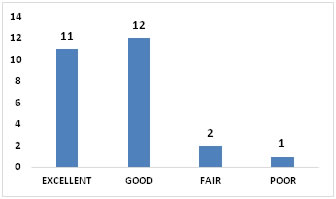
Fracture Union: Average time for radiological fracture union in present study was 16 weeks. Harris Hip Score: Average hip score from the study was found to be 86.04 which ranges from 52 to 95. Functional Outcom: Excellent results were obtained for 11 patients. 12 patients had good results. Fair results were obtained for 2 patients. Functional Outcome of Unstable Inter Trochanteric Fractures: Out of 15 unstable inter Trochanteric fractures, 4 cases had got excellent results and 9 cases had got good results. Functional Out Come of Subtrochanteric Fractures In The Study: Out of 11 cases, 64% had got excellent results after 6 months. (n = 7) Three cases (27%) had got good results.
Figure 1: Functional Outcome DISCUSSION Regardless of the type of fracture, Pertrochanteric femur fractures can lead to substantial morbidity and mortality. Unstable fractures have poor results with the regular methods of fixation. Proximal femur locking plate is an fixed angle stable construct, with locking cancellous screws at 95, 120 and 135 degrees, which can be used in these situations in open as well as minimally invasive per cutaneous plate osteoporosis (MIPPO) technique. The age of the patients ranged from 33 years to 85years, with an average of 67.80 years. The incidence was highest in the 65-85 age group. Among the 26 cases, 62% (n=16) were males and 38 % (n=10) were females. Prakash A Assur and colleagues from Bijapur Karnataka has got a similar sex distribution. 61.7 % (n=21/34) males and 38.2% females (n=13)6. Among the 26 cases, 23 (88%) fractures were sustained as a result of fall whereas 3 (12%) fractures were due to RTA. Most of the patients sustaining peritrochanteric fractures are elderly with osteoporosis and a trivial trauma is enough to cause a fracture in this area. Off the 26 cases, 15 (58%) were unstable intertrochanteric and 11 (42%) were sub trochanteric fractures. Similar results are obtained for Ravi GO andSaheb SH.7. Major co morbidities found among the patients were Diabetes mellitus, Hypertension, Coronary artery disease, Tuberculosis and COPD. This is comparable with present scenario of Kerala population. Average hospital stay duration was 21.5 days. 10 days of post-operative care is given for all cases before discharge. Some pre-operative stabilization was required for patients with co morbidities. Only two patients (8%) developed post-operative complications. One patient developed superficial infection and one patient developed deep infection. Most of the fractures (92%) united without any complication. No mortality was reported during the 6 months follow up period. Average operation time was 88.5, which ranges from 70 minutes to 120 minutes, excluding the time for anesthesia and draping. Average blood loss in the study was 300 ml which ranges from 150 ml to 450 ml. Post-operative transfusion was given for 14 out of 26 cases and intra operative transfusion was given for 3 out of 26 patients. Average hip score from the study was found to be 86.04 which ranges from 52 to 95. Excellent results were obtained for 11 patients. 12 patients had good results. Fair results were obtained for 2 patients. Poor outcome was obtained for a single case. Similar studies were conducted all around the world and most of them concluded with a satisfactory post-operative result. Ravi GO and Saheb SH obtained an excellent result for 48% cases and good result for 38% cases.7 Wei Ting Lee et al got a satisfactory result for 73 % of cases in study conducted in Singapore.8 A study conducted by Hossain MM et al in Dhaka, Bangladesh obtained a very good functional outcome for their patients with an average Harris Hip Score of 92.05.9 A study conducted by Prakash et al in Karnataka obtained an excellent result for 38% cases and a good result for 53% cases.6 Following conclusions are drawn from the study.
LIMITATIONS AND RECOMMENDATIONS
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.