 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 5 Issue 1 - January 2018
A rare presentation of simultaneous four Carpometacarpal joint dislocations: A case report
Aravindan Tharakad Satchidanandan1, Ganesh Babu2*
1IIIrd Year Resident, 2Associate Professor, Sri Ramachandra Medical College and Research Institute, Porur, Chennai-600116, Tamil Nadu. Email: aravindan.tharakad@gmail.com
Abstract Background: Chronic Kidney Disease is a global threat to health particularly for developing countries, since therapy is expensive and life-long.19 Incidence of CKD has doubled in the last 15 years.19Accurate creatinine measurement is essential in the diagnosis of chronic kidney disease as serum creatinine is used for estimating glomerular filtration rate. The aim of our study was to compare the analytical performance between the enzymatic method and compensated Jaffe method for estimation of creatinine. Methods: In our study we measured serum creatinine in 135 serum samples by both enzymatic and compensated Jaffe methods using Cobas c311 automated analyser. Results: Relationship between both the methods using Cobas c311 automated analyser showed a correlation coefficient of 0.999, which means these two methods correlate very well. Conclusion: There was a good agreement and comparability between compensated Jaffe and enzymatic methods except for a minimal variation at higher concentrations of creatinine. Key Words: Creatinine, Compensated Jaffe, Enzymatic method.
Hand injuries vary from simple fractures to complex intraarticular multiple joint injuries. Injuries that include soft tissue involvement may result in delaying prognosis and expected outcomes. Such injuries are carpometacarpal joint dislocations. Carpometacarpal joint dislocations are a rare injury encountered in Orthopaedic practice. The joints movements are gliding in character with strong volar and dorsal ligaments acting as supports, hence they rarely tend to dislocate. It can present involving one or multiple joints of hand as a result of high velocity injury. Carpometacarpal dislocations are at times missed due to diffused edema or inadequate imaging techniques. Multiple dislocations of these joints when managed immediately result in good functional result, hence early intervention is essential.
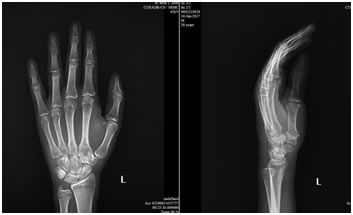
CASE REPORT Right hand dominant, 20 year old male was brought to the casualty following a skid and fall from his motorbike. Falling on an outstretched hand on a median, he complained of pain and swelling over his left hand. With no other long bone injuries or associated head injury, clinical examination revealed diffused swelling with minor abrasions over the dorsum and marked dorsal prominence over the middle third of the hand. Tenderness was elicited over the area of prominence with a bony step and over the ulna styloid. [Figure 1]: Radiograph showed dislocation of the second, third, fourth, and fifth carpometacarpal joints with a communited ulna styloid fracture of the left hand. CT scan of the left hand was done which confirmed the same and showed subluxation of the ulnocarpal and distalradiocarpal joints. Closed reduction under sedation was attempted however reduction was unsatisfactory. Figure 1: X-ray showing 2, 3, 4, 5th CMC Joint dislocation with associated Ulna styloid fracture with DRUJ disruption
Figure 2: CT 3D Reconstruction imaging [Figure 2]: Patient was started on anti-inflammatory and analgesics to reduce soft tissue edema. Patient underwent open reduction internal fixation with k wires and dorsal capsular repair of the second, third, fourth, and fifth carpometacarpal joints with k wire fixation of the ulna styloid. Patient’s hand was immobilised with a well moulded plaster slab over the volar aspect of the hand for duration of 3 weeks, and converted to cast for 3 more weeks. [Figure 3]: Cast and k wires were removed after 6 weeks and active finger and wrist flexion extension exercises were taught. X-rays after 1 month of surgery showed satisfactory reduction of the carpometacarpal joints and healed ulna styloid. Patient was reviewed in outpatient basis and functionality was assessed. Figure 3: Postoperative X ray
Figure 4: 3 months Post op x-ray.
[Figure 4]: After 3 months of follow up QuickDASH score was used to assess the functionality of the hand and wrist, which revealed excellent functionality to near normal. Grip strength and pinch strength were also near normal.
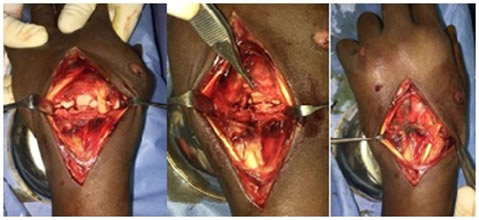
DISCUSSION Dislocations of the first carpometacarpal joint are relatively common, whereas dislocations of the other joints are rare. Though closed reduction and manipulation of the joint is simpler in acute cases1 the biomechanics of the joint is disrupted. Carpometacarpal joints are stabilised by articular capsules and strengthened by the stronger dorsal carpometacarpal ligaments with the second, third and fourth having two ligaments (transverse and longitudinal) whereas the fifth having only one. This adds to the stability of the joints hence and allows movement to occur in a gliding nature. Although the dorsal ligaments are stronger, dorsal dislocations have higher incidence because of the mechanism of injury and volar surfaces of the joints buttress one another2. Figure 5: CMC Joint exposed with torn dorsal capsules identified and sutured [Figure 5]: However the disruptions of both the transverse and longitudinal arches of the hand result in gross morbidity later3. Previously, case series of similar dislocation pattern found closed reduction to be successful in acute dislocations, resulting in good grip and pinch strength but some associated ulnar nerve injury4. In a similar case report with dislocation of all five carpometacarpal joints, close reduction with k wire fixations of the joints was done resulting in 50 degrees of dorsiflexion and 40 degrees of palmar flexion was achieved within one month of follow up5 however functionality in the form of pinch and grip strength were not assessed.
CONCLUSION Open reduction techniques used in carpometacarpal dislocations have been described to be ideal line of treatment in acute injuries, however the repair of vital joint stabilising structures like the dorsal capsule have not been addressed. By repairing the dorsal capsule we have come to understand it not only re-establishes the stability but results in good functional outcome. Since carpometacarpal injuries are rare, open reduction techniques with emphasis on dorsal capsule repair need to be practiced in similar injuries for the ideal outcome.
REFERENCES
|
|



 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.