 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 5 Issue 1 - January 2018
A study of functional outcomes following open reduction and internal fixation of clavicle fractures at kodagu
Mozimul Haq Siddiqui
Assistant Professor, Department of Orthopaedics, Kodagu institute of medical sciences, Madikeri, Karnataka, INDIA. Email: mozimuls@gmail.com
Abstract Background: Fracture clavicle is a common bone injury due to its superficial location in the human body, making it one of the least-protected bones by muscle or fat. Fracture clavicle can be treated either conservatively or operatively depending on the type of fracture. All methods used for treatment of displaced fractures of midshaft clavicle have shortcomings. The present study aimed to assess the functional outcomes following open reduction and internal fixation of clavicle fractures at kodagu . .. Material and Methods: A total of 45 patients aged between 20 and 60 years with mid shaft clavicle fractures that were completely displaced, comminuted or with shortening of more than 15 mm (in comparison to normal side) were operated with locking pre-contoured plate using standardized protocol. Patients were followed up to 6 months of surgery to assess functional outcome by using Neer shoulder score. Results: Among 45 patients, 42(93.3%) fractures united at an average of 12 weeks. 2(4.44%) patients had delayed union and fracture united at the end of 24 weeks, 1 (2.22%) patient had non-union, fracture not united even after 6 months. The functional outcome was assessed by Neer Shoulder Score. Most of the patients i.e., 38(84.4%) had excellent functional outcome, 4 (8.88%) patients had satisfactory result, 2(4.44%) patients had unsatisfactory result and 1 had failure. Conclusion: The success of open reduction and internal fixation for middle third fractures of clavicle requires careful assessment of fracture pattern, patient selection and early mobilization. Functional outcomes were found to be better with operative management of middle third clavicle fractures with locking compression plate. Key Words: Fracture clavicle, open reduction, internal fixation, union, functional outcome.
INTRODUCTION The clavicle, a relatively thin bone, forms the only direct link between the axial and appendicular skeletons1.Fracture clavicle is a common bone injury due to its superficial location in the human body, making it one of the least-protected bones by muscle or fat2.Fractures of clavicles are more common in young active adults with common causes being motor vehicle accidents and sports injuries when falling directly onto the shoulder with the arm by the side3. It accounts for approximately 5% to 10% of all fracture and up to 44% of injuries of shoulder girdle. Around 80% to 85% of clavicle fractures occur in mid-shaft of the bone and result in bony failure. Distal third accounts for 20% and medial third fracture are rarest 5%2-4. Fracture clavicle can be treated either conservatively or operatively depending on the type of fracture. All methods used for treatment of displaced fractures of midshaft clavicle have shortcomings. Conservative treatment of displaced fracture clavicle leads to shortening of clavicle, pain, loss of strength, rapid fatigue, hyperaesthesia of the hand and arm, difficulty sleeping on the affected side and aesthetic complications5-7.More than 9.7% shortening of clavicle of its original length is associated with poor outcome8. High rate of malunion and non-union have been reported with displaced fracture treated conservatively6,9. Operative treatment is considered to be better than conservative in cases of displaced or comminuted fractures5. But every fixation method has associated complications such as neurovascular injury, infection, poor cosmesis due to postoperative scar, resurgery to remove plate, and even non-union after plating5,6,10.Several studies have examined the safety and efficacy of primary open reduction and internal fixation for completely displaced midshaft clavicular fracturesand have noted high union rate with a low complication rate11.The present studyaimed to assess thefunctional outcomes following open reduction and internal fixation of clavicle fractures at Ashwini hospital,Madikeri . ..
MATERIAL AND METHODS The present study was carried out over a period of one year in at kodagu,karnataka. All cases were operated at Ashwini hospital madikeri during 2016-17.During the study period 45patients with midshaft clavicle fractures were treated with open reduction and internal fixation. Inclusion Criteria All male and female patients aged between 20 and 60 years with midshaft clavicle fractures that were completely displaced, comminuted or with shortening of more than 15 mm (in comparison to normal side) were included after obtaining informed consent. Exclusion Criteria Patients aged below 20 and above 60 years with open fracture, pathological fracture, undisplaced fracture, fracture of medial or lateral ends, neurological injury, patients not willing for surgery, patients medically unfit for surgery were excluded from the study. A detailed history was elicited regarding mode of injury, site of pain and swelling over the affected clavicle. Past medical illness and family history were also noted. All the included patients were operated with locking pre-contoured plate using standardized protocol. Postoperatively all patients were put on injectable antibiotics, analgesics and arm pouch. On the 3rd post-operative day, primary wound inspection was done. Patients are discharged after 5 days of uneventful post-operative stay in hospital. Sutures were removed on 10th post-operative day. Patients were followed up after one month, 6 weeks, 3 months, 6 months of surgery to assess functional outcome by using Neer shoulder score. RESULTS The present study included 45 patients of fresh middle third clavicle fracture which was treated surgically with open reduction and internal fixation with plate and screw in Ashwini hospital,madikeri. Majority of the patients i.e. 21 patients (46.6%) were in the age group of 20-30 years followed by 12 (26.6%) patients between 31-40 yrs of age group. Out of 45 patients, 34 (75.5%) were males and 11 (24.4%) were female. In all patients, results were analyzed both clinically and radiologically during regular follow up. Among 45 patients of midshaft clavicle fracture,22 patients (48.8%) had road traffic accident, 13 patients (28.8%) had fall on outstretched hand,8 patients (17.7%) had simple fall on shoulder after slipping and2 patients (4.44%) had fall from height. All fractures in study were classified according to Robinson’s classification. Group 1 Allman fracture of clavicle is Type-2 Robinsons, which is further classified into A1, A2, B1, and B2. In present study, maximum patients i.e., 34 (75.5%) had Type 2-B1 fracture followed by 6 patients (13.3%) of Type 2-B2 (Table 1).
Table 1: Classification of clavicle fractures according to Robinson’s classification
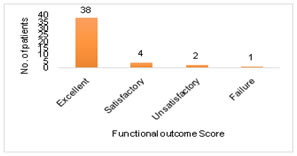
Fracture was considered united when clinically there was no tenderness, radiologically fracture line was not visible and full unprotected function of the limb was possible without any sign of instability and pain. Among 45 patients with middle third clavicle fracture treated with locking compression plate and screws, 42(93.3%) fractures united at an average of 12 weeks. 2(4.44%) patients had delayed union and fracture united at the end of 24 weeks, 1 (2.22%) patient had non-union, fracture not united even after 6 months. Excellent results were seen in most of the clavicle fractures who had complete, painless shoulder range of movements by three months. One patient who had poor result is due to loosening of plate and the patients had some pain over the shoulder in overhead activities and decrease in strength in shoulder abduction. The functional outcome was assessed by Neer Shoulder Score. Most of the patients i.e., 38(84.4%) had excellent functional outcome, 4 (8.88%) patients had satisfactory result, 2(4.44%) patients had unsatisfactory result and 1 had failure (Graph 1). Figure 1: Assessment of functional outcome DISCUSSION Fractures in the middle third of the clavicle represent 80% of all clavicular fractures1,2. Although clavicle fractures usually unite uneventfully with treatment, they can be associated with different outcomes. In present study, fracture of clavicle was commonly occurred i.e., 21 patients (46.6%) in the age group 20-30 year and majority 34 (75.5%) were males. Bostman et al observed average age of 33.4 year and also commonly male were affected 76 patients (74%) compared to female 27 patients (26%)12. Ethiraj et al and Pillai et al also observed 68.3% and 44% of patients in the age group of 19 to 29 years in their studies respectively13,14. Clavicle fractures are traditionally treated conservatively as most of the un-displaced and uncomplicated fractures unite uneventfully but surgery is indicated at the first place in open fractures, floating shoulders, and fractures associated with neurovascular injuries. Surgery should also be considered for fractures which are grossly displaced and severely comminuted as they have propensity to land up in non-union. In present study, 45 were operated by open reduction and internal fixation with plate and screws to analyse the functional outcome. Robinson et al3, Hill et al6 and Nordqvist et al7conducted studies to analyze the results of conservative treatment andfound poor results in displaced middle third clavicle fractures. Bostman et al12 treated 103 cases of middle third clavicle fractures by early open reduction and internal fixation with plate and screws. In present study also 93.3% fractures united at an average of 12 weeks. In Bostman et al12and Ethiraj et al13study, 90% fractures united at end of 12 weeks. In a study by Pillai et al1496.7% fractures were united between 12-14 weeks. When functional outcome was assessed by Neer Shoulder Score, it was found that most of the patients i.e., 38(84.4%) had excellent functional outcome, 4 (8.88%) patients had satisfactory result, 2(4.44%) patients had unsatisfactory result and 1 had failure. Study by Pillai et al14 showed excellent result in 80% patients, satisfactory result in 13.33%, unsatisfactory in 3.33% and failure in 3.33% patients. Ethiraj et al13showed excellent results in 46 Patients (76.7%) and good functional outcome in 10 (16.7%)patients, fair functional outcome in 3 (5%) patients and poor functional outcome in 1 patient. The study indicates that the use of rigid internal fixation and early mobilization in displaced clavicle fracture gives immediate pain relief and prevents the development of shoulder stiffness and non-union. The success of open reduction and internal fixation for middle third fractures of clavicle requires careful assessment of fracture pattern, patient selection and early mobilization. Functional outcomes were found to be better with operative management of middle third clavicle fractures with locking compression plate.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.