 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 5 Issue 3 - March 2018
The operative treatment of displaced middle one third clavicle shaft fracture: Experience of 30 cases
Amol Babasaheb Parturkar1*, Bipin Theruvil2
1Sahyog Nagar, east, new D.P. road, Beed, Maharashtra, INDIA. 2Lakeshore Hospital, Kochi, INDIA. 3Orthopedics Registrar, M T Agarwal hospital, Mulund Mumbai, Maharashtra, INDIA.
Abstract Background: Clavicle fracture is a common traumatic injury around shoulder girdle due to its subcutaneous position. Open reduction and internal fixation can be achieved with intramedullary devices or plate fixation. Aim: To study the functional outcome of surgically treated acute displaced middle one third clavicle shaft fractures with plate and screws. Material and Methods: In this study 30 patients with middle one third clavicle shaft fractures were included who underwent open reduction and internal fixation. In 15 patients anatomically contoured locking compression plate, in 11 patients simple straight locking compression plate, in 3 patients dynamic compression plate and in 1 patient reconstruction plate was used. Results: Average duration for union of clavicle fracture was 12 weeks which includes 2 cases with delayed union. One patient with delayed union resulted in plate breakage which united after replating and bone grafting. Functional outcome after union of surgically treated middle one third clavicle shaft fractures was excellent in 23 patients, good in 5, and fair in 2 patients by Constant and Murley Score. Conclusion: Surgical treatment of middle one third clavicle shaft fractures with plate and screws gives immediate pain relief, early resumption of work and avoids complications like malunion and nonunion. Key Words: Clavicle, middle one third shaft fracture, displaced, open reduction, internal fixation.
Clavicle fracture is a common traumatic injury around shoulder girdle due to its subcutaneous position. Fracture of the clavicle accounts for approximately 5 to 10% of all fractures and up to 44% of injuries to the shoulder girdle. About 70% to 80% of these fractures are in the middle third of the bone and less often in the lateral third (12% to 15%) and medial third (5% to 8%)1. It is caused by either low-energy or high energy impact. Traditional trend of clavicle fracture management was conservative.2 Although many methods of closed reduction have been described, it is recognized that it is practically impossible to maintain the reduction and a certain amount of deformity and disability is expected in adults.1 In the past few years several publications have described about poor outcomes like malunion and nonunion (15%) after conservative treatment of severely displaced clavicle fractures.3,4 In proven cases of nonunion of clavicle fractures, the main treatment modality is open reduction and internal fixation and bone grafting. Open reduction and internal fixation can be achieved with intramedullary devices or plate fixation. In intrameduulary fixation satisfactory rotational stability was not achieved and immobilization for longer period was required. Complications like loosening and breakage of pins were common. The main advantage of early fixation of fresh clavicle fractures is to prevent complications like malunion and nonunion. Accurate reduction and rigid fixation has been reported to provide early pain relief and functional recovery5.The purpose of this study on clavicle fractures is to study the functional outcome of surgically treated acute displaced middle one third clavicle shaft fractures with plate and screws.
MATERIAL AND METHODS This prospective observational study was carried out on 30 patients who sustained clavicle midshaft fractures and were treated surgically with open reduction and internal fixation over a period of one year and followed up for next one year. Inclusion Criteria
Exclusion Criteria
General condition of the patients was assessed and local examination was done. Methodology: All patients were operated under general anaesthesia. After minimal soft tissue and periosteum dissection, fracture fragments were reduced and fixed temporarily with Kirschner wire and then plate was applied over the superior aspect of the clavicle.(Lag screw was put wherever possible and then plate in neutralization mode was applied).While drilling from superior to inferior direction, a periosteal elevator was inserted inferiorly to prevent the drill from damaging the important neurovascular structures inferiorly. The medial and lateral fracture fragments were fixed with the plate with 3.5mm cortical and lockin screws depending upon the fracture morphology. At least three screws were put on either side of the fracture. Wound was closed in layers after ensuring proper hemostasis and sterile dressing was applied and broad arm sling was given. After surgery limb was immobilized in a broad arm sling with shoulder held in adduction and internal rotation. Elbow was maintained at 90° of flexion. Rehabilitation protocol was planned depending upon the stability of fixation. For well-fixed and stable fixation, active assisted range of motion of shoulder joint was allowed up to 90 degrees of abduction and flexion,45 degree of external rotation. After 6 weeks, patient was reassessed with X-ray and active range of motion in all planes were allowed. At eight to 12 weeks, isometric and isotonic exercises were prescribed to the shoulder girdle muscles. In comminuted fractures and fractures which were not rigidly fixed, range of movement exercises were delayed. Patients were followed up as outpatient basis with X-ray after 6 weeks, 3 months, 6 months and 1 year from the date of surgery. Clinical evaluation will be done by Constant and Murley scoring system.6
Figure 1: Reduction of fracture fragments and fixation with plate and screws on superior aspect of clavicle. RESULTS Majority of the patients studied were of the age group 16-29 (14) that is 46.6%. 27 patients (90%) were males and 3 patients (10%) were females. In middle third shaft clavicle fractures, 21 patients (70%) had road traffic accident, 4 patients (13.3%) had simple fall on shoulder, 5 patients (16.6%) had fall on outstretched hand. 25 patients (83.3%) had direct injury to shoulder and 5 patients (16.6%)had indirect injury to shoulder. There were 17 patients (56.6%) who were classified as type 2B 1, 12 (40%) as type 2B 2 and one (3.3%) as type 2A 2.The most commonly used implant was anatomically contoured LCP which was used in 15 patients (50%), followed by simple straight 3.5 LCP which was used in 11 patients (36.6%) (Table 1).
Table 1: Types of plates
For type II A 2, one one simple LCP was used. For type II B 1, 1 DCP, 8 anatomically contoured LCP and 8 simple LCP were used. For type II B 2, 1 reconstruction plate, 2 DCP, 7 anatomically contoured LCP and 2 simple LCP were used.
Table 2: Complications
In middle third clavicle fixation 6 patients had hypertrophic skin scar and in 5 patients plate prominence occurred out of which one underwent implant removal. In 2 patients delayed union occurred. In 1 patient delayed union lead to plate breakage.1 patient (3.3%) restriction of shoulder movements occurred. This was because of the reason that patient had sustained head injury and so was not compliant with physiotherapy protocol. Movements were improved once patient was recovered from head injury and underwent proper physiotherapy. Functional outcome was assessed by Constant and Murley Score System (Table 3).
Table 3: Functional outcome
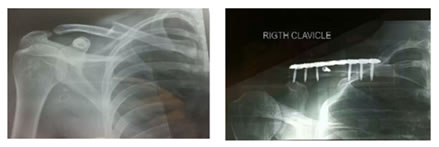
Figure 1: Figure 2: X-ray - Preoperative and after one year Figure 3: Functional outcome after one year DISCUSSION Average age of the study group was 37 years, with standard deviation of 14.5yrs. In Bostman et al study patients average age was 33.4 years and commonly males were affected that is 76 Patients (73.79%) compared to females 27 patients (26.21%).7In this study there were 17 patients (56.6%) who were classified as type 2B 1, 12 (40%)as type 2B 2 and one (3.3%)as type 2A 2.In Bostman et al study also Robinson type-2B1 was common in 81 patients (78.64%). Robinson type-2 B2 occurred only in 22 patients (21.36%).7 In this study most commonly used implant was anatomically contoured LCP which was used in 15 patients (50%), followed by simple straight 3.5 LCP which was used in 11 patients (36.6%). This is in comparison with Bostman et al study where reconstruction plates were used in 46 patients (44.6%).7 Dynamic compression plates were used in 55 patients (53.40%)and semi tubularplatesin2patients (1.94%). In the initial period of his study dynamic compression plates were used then in later part of his study reconstruction plates were used. He found no difference in the complication rate between the patients treated by dynamic compression plate and reconstruction plate. In this study, the most commonly used was 7 holed plate in 16 patients (53.3%), 6 holed plate was used in 12 patients (40%) and 8 holed was used in 2 patients (6.6%).In Bostman et al study plate length was above 6 holes to place at least three screws in each fragments. Plate length also depends upon the amount of comminution.7 In middle third clavicle fracture 28 fractures (93.3 %) united at or before three months. 2 patients (6.6%) with delayed union underwent bone grafting. 1 patient with delayed union had plate breakage. Shen WJet al in their stated radiological union occurred approximately between 6 to 12 weeks.8 One patient (3.3%) plated with reconstruction plate for Robinson type 2 B 2 fracture had plate breakage in postoperative period. He was reoperated with anatomically contoured LCP with bone grafting. This fracture united at 20 weeks postoperatively. In Bostman et al study 2 patientstreated with semi tubularplate had implant breakage at 2nd and 7th postoperative weeks respectively.7 Both cases were treated by replating using dynamic compression plate with bone grafting. Two patients (6.6%) had delayed union. One case of delayed union resulted in plate breakage for which replating and bone grafting was done. It united at the end of 20 weeks. For second patient with delayed union bone grafting was done which united at 16 weeks. In Bostman et al study delayed union occurred in 3 Patients (2.91%).7Olivier V Erborgt et al reported the surgical outcome after open reduction and plate fixation of middle-third fractures of the clavicle in 39 semi- professional athletes. Wound infection was seen among 18% of the cases, 5% of the cases had nonunion, 7% of the cases had neurological symptoms and 5% of the cases had refracture.9 In this study on 30 patients with middle third clavicle fracture treated with plate and screws 23 patients (76.6%) had excellent functional outcome, good functional outcome in 5 patients (16.6%) and fair functional outcome in 2 patients (6.6%) who had restricted shoulder ROM and plate loosening. In a study by Agarwal et al, among 17 cases with 4 to 5 weeks time to return to functional range, 14 cases had excellent outcome and among 13 cases with 6 to 8 weeks time to functional range, 9 cases had excellent outcome. This study showed that the most important advantage of open reduction and internal fixation of clavicle fractures of middle one third shaft was early pain relief and resumption to normal work.
REFERENCES
|
|



 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.