 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 6 Issue 2 - May 2018
Treatment of aseptic nonunion of tibia study of 35 cases by ilizarov ring fixator: A prospective clinical study
V R Rokade*, Pankaj Lawate**, Anant Chowgule***
*Associate Professor, ** Sr. Resident, *** Assistant Professor, Department of Orthopedics, Government Medical College Miraj, Maharashtra, INDIA. Email: drvikas852@gmail.com
Abstract Objective: To achieve union at nonunion site with correction of limb length discrepancy and correction of deformity with early function and mobilization. Methods: It is prospective study of treatment of aseptic nonunion of shaft tibia. Total 35 patients of tibial nonunion were studied. All relevant pre and perioperative information and complications were recorded. Also assessment of functional outcome was made. Results: In present series 32 out of 35 cases has united, about 91% success rate. The average duration of nonunion was about 14.5 months, average union time (fixator removal) is about 6.2 months. Two of our patient were showing poor tolerance to ilizarov external fixator changed to other modality. Conclusion: Ilizarov technique is very helpful in treating nonunion of long bones and has advantage of early wt. Bearing, movements of nearby joints encouraged which reduces edema and joint stiffness. Key Words: Aseptic nonunion, Ilizarov ring fixator.
INTRODUCTION There are many modalities of treatment of aseptic nonunion of shaft tibia, which have evolved during last so many years, all aims at achieving the common goal of union of fracture and restoration of function. Management of nonunion shaft tibia has been described as difficult and discouraging because of lesser blood supply to area owing to anatomical location where there is less muscular attachment. Improvement in internal fixation system have proved sufficiently stable fixation to allow active and passive range of movement of adjacent joint but ILIZAROV external fixator continues to be an effective and versatile method for the treatment of difficult nonunions5,6. Ilizarov method is axially elastic and allows weight bearing and function, which is important for union, it corrects associated deformity 3,4.
MATERIAL AND METHOD A study of 35 cases of aseptic non-union shaft tibia in adults by ilizarov external fixation was done in 3 years. Period of study was in between March 2013 to May 2016. Duration for Follow up ranged from 2 to 4 years. All the patients were hospitalized and managed according to a standard protocol, which include preoperative evaluation starting of compression distraction osteogenesis after stitch removal. Discharge with advise of compression distraction follow up on OPD basis. PREOPERATIVE PLANNING(3,4): Each case of non union was classified according to AO and Paleys classification, orientation of non union with special consideration to atrophic / hyper tropic/ gap non union/ need of corticotomy for shortening keeping the preconstruct ready. All required blood investigations and radiographs were done. Physician fitness taken. Operative Procedure: Atrophic nonunion:- Under IITV control fracture site is exposed bone ends are visualized shingling is done upto 2to3cm on either side freshening done till unctuate bleeding appears (i.e. paprika sign) after release of tourniquet medullary canal on both the fragment are reamed and cancellous bone grafts are placed taken from iliac crest. Fibulectomy It is done about 8 cm above the lateral malleolus. Hypertropic nonunion: - Ilizarov frame applied and nonunion site stabilized for compression distraction osteogenesis. Oligotrophic nonunions :- Requires exploration of nonunion site reaming of canals freshening bone grafting and external stabilization Application Of Ilizarov Ring Fixator: A four ring preconstruct6 inserted in leg under IITV pass a reference wire at proximal tibial level parallel to the joint using tibial safe zones and fix it to the first ring, then pass a K wire in to the distal tibia 2 cm proximal to joint line and fix it to the distal ring. Then pass another wire from the proximal tibia making maximum possible angle to the reference wire is passed through safe zone, another wire is pass through the fibula before passing this wire just put a thumb over common peroneal nerve to protect it and displaced it away from the course of wire fix this two wire to the proximal tibial ring, then another two wires are passed at distal tibial site and fix it to 4th ring, then one K wire is passed in each of fragment and fixed to 2nd and 3rd ring. Insertion of shanz pin - Rancho cubes are attached to the 2nd and 3rd ring in such a way that they are at anteromedial surface of the tibia and6 mm tapered shanz pin is passed and fixed to rings. CORTICOTOMY- It is defined is sectioning of cortex of bone at the same time preserving the periosteal and nutrient artery intrigity supplying the medullary canal7,10. In some cases of paley's type B2 and B3 patient required a proximal tibial corticotomy. Post Op. Management- Day 1: Walking with walker full weight bearing., dorsiflexion by alkathien foot plate. And movements of toes, ankle and knee joint. Day 3: Corticotomy dressing 2)Daily wire and pin track care Day 7: Starting of compression at fracture site and distraction at corticotomy site @ 0.25mm four time a day. Day 12: Suture removal. Day 14: Check x-ray for fracture site and corticotomy site. Discharge patient with following instruction Distraction at corticotomy and compression at fracture site. Daily wire tract dressing, physiotherapy, report immediately if pain or wire breakage. Follow up visit after 15 days. Follow Up Visit Following things were checked
Criteria for Assessment Of Results4,7,10 Satisfactory results
Functional Results
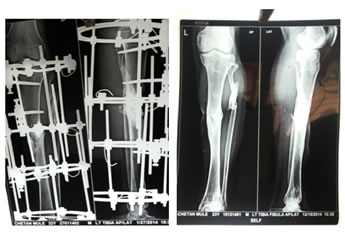
Figure 1:
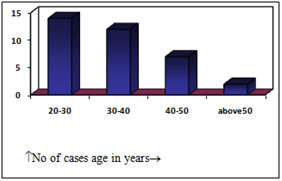
OBSERVATION AND RESULTS Table 1: Age distribution
Figure 2:
Table 2: Sex distribution - Table no 1
Table 3: Side of nonunion - Table no 2
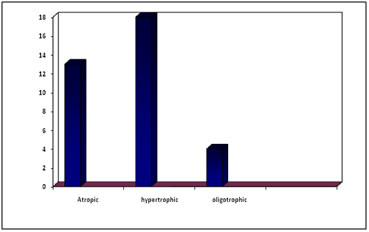
Table 4: Type of nonunion according to weber classification (10) -Table no 3
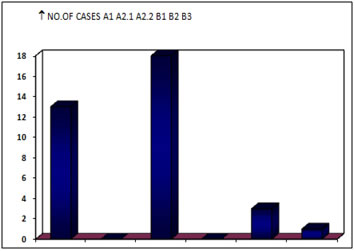
Table 5: Type of nonunion according to paley’s classification3,4 Table no 4
Figure 3: Figure 4:
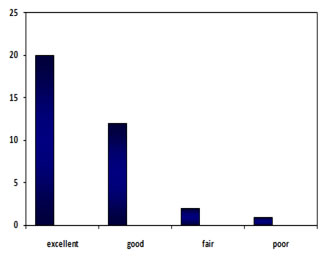
Table 6: Results Table no 5
Excellent to good results were seen in 91.42% of cases
Figure 5:
Table 7: Comparative series (9) Table no 6
DISCUSSION Nonunion of shaft tibia is more common than nonunion of any other long bone in the body; this is because of lack of soft tissue surrounding the tibia and the subcutaneous nature of the tibial fractures being compound. Inspite of many modalities for the treatment of aseptic nonunion of shaft tibia ilizarov external fixator in treatment of choice and a versatile modality of treatment the existing orthopaedics literature has recorded widely varying results2,11,12. This present series of treatment of aseptic nonunion of shaft tibia by Ilizarov external fixator has been aim to try and reduce morbidity this series has 35 cases of aseptic nonunion shaft tibia in adults by ilizarov external fixator. This series has got 18 cases out of 35 cases (52%) of hypertrophic nonunion 13cases i.e. (37%) of atrophic nonunion 4 cases i.e. (11%) of oligotrophic nonunion. Among these cases majority of the cases i.e. 26cases out of 35 cases were in the age group of 20-40 years (75%) youngest patient being of 20 years As the tibial fractures are associated with road traffic accidents majority of nonunions were males about 29 cases out of 35 cases i.e. 83% are males. Right and left side were in the proportion of 3:2 i.e. left 60% right 40% About 22 cases out of 35 cases i.e. (63%) were having closed fractures and 13cases out of 35 i.e. (37%) were having compound fractures. Majority of cases i.e.26cases out of 35 cases (75%) were treated in one or the other modality of surgery and rest of i.e. 9 cases (25%) were treated in the form of above knee cast. According to paley’s classification3,4,10 amongst type –A 13 cases out of 35 i.e. (40%) were type A1 and 18 cases out of 35 i.e. (51%) were type A2.2 i.e. stiff nonunion without deformity. Average duration of nonunion is about 14.5 months longest being 72 months and shortest being 4 month. All the patients were treated with standard protocol given pre operative antibiotic. For the atrophic nonunion cases we have explored the fracture site removed all fibrous tissue at the fragments done freshening / shingling iliac crest bone grafting fibulectomy if it is united and stabilized it with a four ring ilizarov external fixator. In the Gonzalez series9 39 out of 45 cases about 86.66% has united his average duration of nonunion was 10.7 months His average union time was 5.4 months none of his cases has required bone graft 4 of his patients were showing poor tolerance to external fixator one of his case required tendo Achilles lengthening. In present series 32 out of 35 cases has united, about 91%. The average duration of nonunion was about 14.5 months average union time (fixator removal) is about 6.2months 2 of our patient were showing poor tolerance to ilizarov external fixator. All atrophic cases about 13 were augmented with cancellous bone graft none of the hypertrophic nonunion cases were explored In 4 oligotrophic nonunion cases only fracture site was explored and intramedullary canals were reamed and stabilized with ilizarov ring assembly. Six of our cases developed superficial pin tract infection, which was tackled with oral antibiotics and local injection of gentamycin with no further complication. Two of our cases were showing signs of persistent nonunion clinically as well as radiologically were later on treated with locked intramedullary nailing which later on united solidly. One case developed intramedullary infection and was converted into infected nonunion which was later on treated with vancomycin impregnated V-nail along with ilizarov assembly which was united solidly along with cure of infection. Complications No surgery is devoid of complication and problems have its share in it. Following Complications are encountered.
CONCLUSION Most important advantage of the ilizarov technique is early wt. Bearing on first post op. day, movements of near by joint is encouraged, which reduces edema and joints stiffness. Ilizarov method offers advantage was that fixator assembly can be later on adjusted in wards. Early ambulation and wt. Bearing reduces the hospitalization as the patient can be discharged early from hospital and treated on OPD basis.
SUMMARY A series of 35 cases of aseptic nonunion shaft tibia treated with ilizarov external fixator were analyzed and followed upto the return of function
REFERENES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.