 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 6 Issue 2 - May 2018
Valgus intertrochanteric osteotomy along with use of dynamic hip screw for fixation of neck femur fractures: An experimental study from Maharashtra
Shekhar Malve1, Ashish Desai2*, Sujay Kulkarni3, Prasad Powar4, Guruchan S5, Prajwal B N6
{1Assistant Professor, 2,3Sr. Resident, 5,6Jr Resident, Department of Orthopedics}, {4Professor and HOD, Department of Physiotherpy} PGI Swasthiyog Prathisthan, Dr. S.G. Kulkarni Hospital Miraj, Maharashstra, INDIA. Email: drdesaiashish@gmail.com
Abstract Background: Various factors affecting the fracture neck femur outcome and the controversies regarding its management has always been a challenge. With advent of the automobile age and the rapid urbanization, road traffic accidents, high velocity trauma has become quite common place in today’s life. As a result fracture neck of femur in young adults is on the rise. Objective: To study the efficacy of Valgus Intertrochanteric osteotomy for fixation of neck femur fractures along with Dynamic Hip Screw as implant for fixation. Methodology: Experimental study conducted by involving 30 patients with fracture neck of femur with various reasons and approaching to our hospital. Results: Mean age of the subjects was 40± 12.2 years. 70% of the subjects had Type III fracture. The difference in the mean Pauwell’s angle was found to be significant after operation. In 90% of cases, union at osteotomy site was seen within 2-3 months and union at fracture site was seen in 53.3% patients within 3-4 months Key Words: fracture neck femur, valgus intertrochanteric osteotomy, dynamic Hip Screw.
INTRODUCTION The fracture of femoral neck has always been called “the unsolved fracture” as described by Dickson and Nicolls because of the various factors affecting its outcome and the controversies regarding its management. Even the joint replacement surgeries, which have heralded a new era in the world of orthopaedic surgery, have not completely solved this problem fracture, which has plagued orthopaedic surgery since its origin. 1 Today joint replacement surgery to a very large extent has solved the treatment dilemma in older individual, whose expected life span will not exceed that of the endoprostheses available today. But this option of joint replacement cannot be offered to younger individuals mostly because the expected remaining life span of these individuals which varies between thirty to sixty years which easily exceeds that of any endoprostheses available today. Also the curtailments of various activities like squatting and sitting cross-legged which are imposed upon a person after joint replacement surgery are not found acceptable in these individuals who usually lead a vigorous life. In the past fracture neck of femur was not to be found commonly in young adults. But with the advent of the automobile age and the rapid urbanization, road traffic accidents and the attendant high velocity trauma has become quite commonplace in today’s life. As a result fracture neck of femur in young adults is on the rise. In the last decade it was felt that arthroplasty especially of the non-cemented variety would provide a standardized and lasting solution to the problem of the intracapsular fracture in the younger individuals. However it is slowly becoming apparent that a complete solution is yet to be found.2, 3, 4 Even today complication rates of various treatment modalities available for fracture neck of femur in young adults remain unacceptably high. It is still proving very difficult to salvage the femoral head in these patients because of precarious blood supply and strong muscle forces acting across this fracture. 5 The results of treatment of these fractures are dependent on 1. Degree of initial displacement, 2.Degree of posterior communition, 3.Degree of vascular impairment, 4.Accuracy of reduction and stable internal fixation, 5.Duration between fracture and fixation. Femoral neck fractures in young adults are associated with higher incidence of femoral head osteonecrosis2-10 and nonunion2,3,6,11. The incidence of osteonecrosis reported in literature ranges from 12-86% in young adults after femoral neck fractures12-14 With this background that we decided to assess the use and efficacy of intertrochanteric valgus osteotomy fixed with dynamic hip screw in 30 cases of neck femur with vertical shear fracture pattern and Garden’s Grade III and IV.
MATERIAL AND METHODS This study pertains to the study of 30 cases of fracture neck of femur which includes 22 cases of fresh fractures and 8 cases of non union .Individuals in age group of 15-65 years with average age of 40 years were treated in this institute from 1st August 2008 to 30th November.2010.There were 20 males and 10 females Inclusion Criteria
Exclusion Criteria
Patients following up less than 3 months. Gardens type I and II are undisplaced or minimally displaced so were excluded from the present study. A retrospective chart review was performed of all patients; all case papers, indoor sheets, patient interviews preoperative and postoperative X-rays, and records were studied. All operated patients were followed up regularly and at timely intervals and repeated radiographic and clinical assessment done. Patients were followed up for an average of 11.3 months. On final follow up visit Harris hip score a measure of the functional outcome was calculated on every patient. The following standard protocol is followed at our institute for fracture transcervical neck femur in young adults:
Clinical evaluation (Following was done)
Preoperative radiological assessment and Classification. (Following was done)
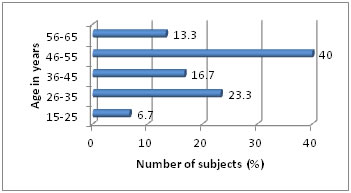
First step is to reduce the fracture anatomically or in valgus position. Angle made by femoral side fracture line with horizontal line is Pauwell's angle (ABC) which opens medially. Wedge (PQR) to be taken from trochanteric area (PQR) is Pauwell's angle minus 30 RESULTS Figure 1: Figure 1: Distribution according to age
Majority of study subjects were from 46 to 55 years of group. (40%) The minimum age of patient was 15 years and the maximum was 62 years. Mean age of the subjects were 40± 12.2 years.
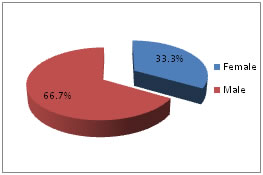
Figure 2: Distribution according to gender Majority of subjects were males i.e. 66.7% Table 1: Classification of fracture-Garden type
Majority i.e. 21(70%) of the subjects had Type III fracture and only 9 i.e. 30% had type IV fracture
Table 2: Comparison between pre op and post operative Pauwell’s angle
Mean Pauwell’s angle before operation was 61± 5.74 degrees whereas it was observed to be 30.37± 5.01 degrees. The difference in the mean angle was compared by using paired t test which was found to be statistically highly significant. It means after the operative procedure the angle was brought down to 30.37 degrees.
Table 3: Comparison between pre op and post operative Pauwell’s angle
Pre operative Pauwell’s angle was (61-65) degree in 43.3% patients followed by (50-55) degree in 23.3%. Post operative Pauwell’s angle was brought down to 26-30 and 31-35 degrees in 30% patients each.
Table 4: Union at osteotomy and fracture site
In majority of cases (90%), union at osteotomy site was seen within 2-3 months and union at fracture site was seen in 53.3% patients within 3-4 months.
CONCLUSION Dynamic hip screw is implant of choice since with lateralization of distal shaft mechanical alignment of limb is maintained and osteoarthritis of knee is prevented. Thus to conclude, an attempt at preservation of the femoral head in fractures of femur neck by adequate reduction and performing intertrochanteric valgus osteotomy internal fixation with dynamic hip screw in properly selected patients can solve the mystery of this unsolved fracture to a great extent
DISCUSSION Optimum valgus position is essential because excessive valgus may cause pressure on the head of femur and avascular Necrosis. And also change in acetabular trochanteric distance may stretch muscles 81. fig DHS has advantage over double angled plate which causes medallization of shaft of femur and strain on knee valgus. Rotational control of the proximal femoral fragment can be difficult to achieve via the insertion of a blade plate and further difficulties can arise during the introduction of the plate into the trochanteric region. Early insertion of the hip screw and use of the barrel and side plate allow for manipulation of the proximal femoral fragment and increased rotational control of the side plate during insertion. Reaming provides internal autogenous grafting of the fracture site and the compression screw component enables the surgeon to maximize compressive forces across the site of nonunion. These features provide advantages for use of the sliding hip screw versus the blade plate Bridge maintainance is important so as to avoid collapse between the entry point and osteotomy site especially in osteoporotic bones. The optimum bridge should be 1 cm to 1.5 cm. Although fracture union was achieved in most of the patients, a persistent limp attributed to loss of femoral offset and abductor moment arm was common. For this the wedge from intertrochanteric region should be difference between current non union verticality and desired horizontality to minimize effect of leg rotation. By producing valgus by Wolfs law induces osteogenesis. Shaft medialisation leads to decrease in offset hence abductor muscle insufficiency and hence limp .It also produces knee valgus so to avoid this lateralisation of shaft is necessary15. Although valgus ostetomy have focused on union rate and progression of osteonecrosis, Literature has been written about clinical function after salvage procedure. Recently Mathews et al15 evaluated the functional outcome in 15 patients with valgus osteotomy for femur neck fracture non union at mean follow up of 4 years after surgery. Although fracture union without progression of osteonecrosis was achieved in most patient persistent limp was noted due to loss of femoral offset and abductor moment axes. Anglen16 reported a series of 13 patients followed-up for a mean of 25months after valgus intertrochanteric osteotomy with a blade plate. All of the fractures healed and 85% of the patients were found to enjoy a good result or better. Marti et al 17 published a larger series of 50 patients, treated with the same method, and found that 86% of the nonunions healed in 4 months. Bartonicek’s18 evaluation of 14 patients treated with intertrochanteric osteotomies and 120-degree blade plates demonstrated a success rate of92%.Ballmer et al’s19 ten series found that 71% of patients healed after an attempt at valgus intertrochanteric osteotomy, whereas Zehi et20 reported only 1 patient in a series of 41 experiencing nonunion. Compared with other methods like Negi use of vascularised21 and non vascularised22 fibular graft which showed 40% and 25% success rate respectively and Bakshi23 mucle pedicle graft which showed 20 % success rate valgus intertrochanteric osteotomy gave us a success rate of 90%.
Table 5: Comparison with different studies
REFERENCES
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.