 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 6 Issue 2 - May 2018
Malleolar fractures of ankle in adults: Functional outcome and complications following open reduction and internal fixation
Ashish Desai1, Shekhar Malve2*, Siddharth Vakil3, Vaibhav Goyal4, Ameya Sawarkar5, Sayali Kalbhor6
1Sr. Resident, 2Assistant Professor, 3,4,5Resident, Department of Orthopedics, PGI Swasthiyog Prathisthan, Dr. G. S. Kulkarni Hospital Miraj, Maharashtra, INDIA. 6Resident, Department of Medicine, SRTR Government Medical College, Ambajogai, Maharashtra, INDIA. Email: shekhardoc82@gmail.com
Abstract Background: Ankle injuries may result from high energy as well as low energy rotational forces sustained during sports or a misstep during routine daily activities.3 Young and middle aged are more prone for this type of injury. Population-based studies suggest that the incidence of the ankle fractures has increased dramatically since the early 1960s. Objective: To evaluate the functional outcome and complications following open reduction and internal fixation of malleolar fractures of ankle in adults. Methodology: The study was a descriptive observational study conducted involving all the adult patients of malleolar fractures. Total of 35 subjects of malleolar fractures undergoing open reduction and internal fixation and fulfilling the eligibility criteria were selected for the study. Results: 31.4% subjects each were from 31-40 and 41-50 years age group with mean age of 39.32 +/- 4.16 years. 37.1% patients had Supination External Rotation and 34.3% patients had Pronation External Rotation type of injury. 82.9% patients had Bi-malleolar fracture. 11(31.4%) patients had excellent outcome. Post-operative complications included superficial skin infections in 17.1% and Ankle stiffness in 5.7% cases. Conclusion: At the end of 6 months, 11(31.4%) patients had excellent outcome, 19(54.3%) had good results, 3 (8.6%) patients had fair outcome while 2 (5.7%) had poor results according to Baird and Jackson score. Weber type B was the commonest type of fracture while supination external rotation injury was the most common mechanism of injury. Key Words: Malleolar fractures, ankle, adults, functional outcome, complications, open reduction and internal fixation.
INTRODUCTION Sir Robert Jones said -Ankle is the most commonly injured joint of the body but the least well treated.1 They are usually mixed injuries, ligamentous and bony and each injury is an end result of the sequence of ligamentous and bony failure due to deforming forces.2 Malleolar fracture have varied presentations which have given rise to a wide variety of classification systems, of which two are Lauge - Hansens and Danis - Weber classification. Ankle injuries may result from low energy rotational forces sustained during sports or a misstep during routine daily activities.3 Young and middle aged are more prone for this type of injury. In the recent times, due to the rapid urbanization and change in life style of the people, the incidence of road traffic accidents are rising rapidly and this tendency will probably continue more so, in the near future. Due to this continued trend, people are sustaining injuries and ankle is the one of the most frequently injured areas of the skeleton. Population-based studies suggest that the incidence of the ankle fractures has increased dramatically since the early 1960s.4,5 The ankle is a complex joint consisting of functional articulations between the tibia and fibula, tibia and talus, and the fibula and talus, each supported by a group of ligaments.5,6 Normally, the ankle joint has 15-20 degree of dorsiflexion and 35-40 degree of plantar flexion. This motion is essential for normal function and anything that reduces this motion will limit function of the entire foot-ankle complex.7,8. Many of the fractures which are stable are reduced by conservative treatment and have given good result. The other unstable displaced and open fractures require open reduction internal fixation (ORIF). The superiority of ORIF over closed treatment has been thoroughly demonstrated in literature.9,10 When malleolar fractures are not reduced accurately they may lead to post-traumatic painful restriction of motion or osteoarthritis or both.11-14 With regard to the treatment, there is still no consensus as to the optimal solution for malleolar fractures. These fractures require anatomical reduction and stable fixation. However, different operative techniques including screw-fixation, buttress plate fixation and ORIF have been adopted by different orthopaedic surgeons. Open reduction and internal fixation is generally the standard of care for unstable ankle fractures. However very few investigators have examined the functional recovery following operative treatment of malleolar fractures. So, the purpose of this study is to assess functional outcome after open reduction internal fixation in these fractures.
MATERIAL AND METHODS The study was a descriptive observational study conducted in Department of Orthopaedics, Post Graduate Institute of Swasthiyog Pratishthan, Extension Area, Miraj involving all the adult patients of malleolar fractures coming to our hospital and fulfilling the eligibility criteria Inclusion Criteria
Exclusion Criteria
Sample size and sample technique: Sample was calculated from following formula: N = Zα2 p (1-p) d2 Z = standard normal variate [at 5% type I error (p < 0.05)] is 1.96 p = Expected proportion in population based on previous studies [54] = 0.047 d = absolute error or precision to be decided by researcher is 0.05 Sample size = 35 Thus a total of 35 subjects of malleolar fractures undergoing open reduction and internal fixation and fulfilling the eligibility criteria were selected for the study. A detailed history was taken and the mode, type of injury was inquired. Patients were examined for other bony injuries and visceral injuries. All the patients included in the study were investigated thoroughly with –
The fractures were then classified as per the Lauge-Hansen’s and Weber’s classification both. All the patients were treated by open reduction and internal fixation once swelling decreased. The patients were followed up at 2nd week, 4th week, 6th week, 3rd Month and 6th month. Post-operative physiotherapy with early range of motion exercise was instituted. At the end of 6 months, patients were evaluated as per the rating of the Baird and Jackson criteria which included objective criteria, subjective criteria and Radiological evaluation. Data Analysis: The quantitative data were represented as their mean ± SD while categorical data was expressed in frequency and percentage. Statistical analysis was carried out by using SPSS software version 21. Quantitative data was presented as mean and standard deviation while qualitative data was presented as frequency and percentages. RESULTS Table 1: Demographic information of study subjects
Majority of the subjects i.e. 31.4% each were from 31-40 and 41-50 years age group. Mean age was observed to be 39.32 +/- 4.16 years. Majority of study subjects were males 23 (65.7%) whereas females were 12 (34.3%)
Table 2: Distribution of subjects based on Lauge Hansen Classification
The mechanism of injury was classified based on Lauge - Hansen classification, in which 13 (37.1%) patients had Supination External Rotation, 12 (34.3%) patients had Pronation External Rotation, 8 (22.9%) patients had Supination Adduction and 1 patient each had Pronation Abduction and Pronation Dorsiflexion type of injury each respectively.
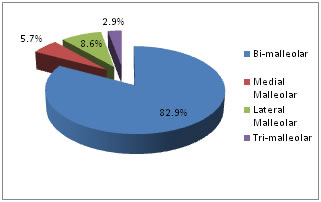
Figure 1: Distribution according to type of malleolar fracture
In our study, 29 (82.9%) patients had Bi-malleolar fracture, 2 (5.7%) had Medial malleolus fracture, 3 (8.6%) had Lateral malleolus fracture and 1(2.9%) patient had Tri-malleolar fracture.
Table 3: Distribution of subjects according to functional outcome
Functional outcome was assessed by using Baird and Jackson score. At the end of 6 months, 11(31.4%) patients had excellent outcome, 19 (54.3%) had good results, 3 (8.6%) patients had fair outcome while 2 (5.7%) had poor results.
Table 4: Distribution of subjects according to complications
There were no cases of intra operative complications. Post-operative complications included superficial skin infections (6 cases, 17.1%) and Ankle stiffness (2 cases, 5.7%). DISCUSSION Age Distribution: The age of the patients ranged from 23 to 62 years with the fracture being most common in 3rd and 4th decade and an average age of 39.32 years. The age distribution in present study is in accordance to the previous literature. 15-17 A total of 25 patients of malleolar fracture were studied by Roberts et al.17 with mean of the study group as 40.0 years. Mean age observed in the studies by Beris et al.15 and Maruti CV et al.16 was 30.7 years and 28.8 years. The age distribution in present study as well in other studies in literature shows that malleolar fractures are relatively more common in young adults. Sex Distribution: Male predominance was seen in present study with, 23 (65.7%) males to 12 (34.3%) females. Our findings were comparable with a study conducted by Nabeel Sham et al.12 and Maruti C V et al.16 who also observed male predominance in their series with 62% and 70% male population in total reported cases. This is possibly due to the fact that in India, malesare involved more in outdoor activities like travelling, occupational movements, sports, etc. than females. Type of Fracture: In our study, 29 (82.9%) patients had Bi-malleolar fracture, 2 (5.7%) had Medial malleolus fracture, 3 (8.6%) had Lateral malleolus fracture and 1(2.9%) patient had Tri-malleolar fracture. As per weber's classification 6 (17.1%) had Type A, 19 (54.3%) had Type B and 10 (28.6%) patients has Type C fractures. Listeal et al.15 in their series observed type B as the most common fracture with the prevalence of 64.8%. Hughes et al.17 also observed similar results with 60% cases of type B out of total cases. Type C was observed as the most common fracture in the series by Stufkens et al.18 with 47.7% cases of Type C and 33.9% cases of Type B fractures. Functional Outcome: Functional outcome was assessed by using Baird and Jackson score. At the end of 6 months, 11(31.4%) patients had excellent outcome, 19 (54.3%) had good results, 3 (8.6%) patients had fair outcome while 2 (5.7%) had poor results. In a similar study by Motwani et al. 19 40 cases of bimalleolar fractures of ankle were treated by ORIF. Excellent results were achieved in 23 cases (57.5%), good in 10 cases (25%), fair in five cases (12.5%), and poor in two cases (5%). In a similar study by Shams et al12, out of 21 patients treated, overall good to excellent results were obtained in 17 patients (80.1%). Our findings were also comparable to the study of Maruti et al.16 (Excellent -20%, Good – 70%). Complications: There were no cases of intra operative complications. Post-operative complications included superficial skin infections (6 cases) and Ankle stiffness (2 cases). Six patients who developed superficial skin infections, were treated with daily dressings and appropriate antibiotics after pus culture and sensitivity. All these infections subsided on treatment. Study conducted by Eugene and Beauchamp et al.20 had superficial infections in 9% patients. A similar incidence of SSi was also observed by Carragee EJ et al.21 (9%). We also had 2 patients with ankle stiffness. This was probably due to the noncompliance of the patient to the advised physiotherapy regimen, as there was no means to monitor the physiotherapy of the ankle joint after discharge of the patient.
CONCLUSION Weber type B was the commonest type of fracture while supination external rotation injury was the most common mechanism of injury. Management with open reduction and internal fixation gives excellent results without problems of pain, stiffness, squatting, and activity of daily living. This study recommends that surgical treatment of malleolar fracture is necessary to achieve anatomical reduction of the fracture fragments, ankle mortise congruity, restoration of the length of the fibula and restoration of syndesmotic integrity. Fracture must be fixed as early as possible preferably within 24 hours or once swelling decreases to prevent post-operative complications like excessive swelling, superficial infection. We also recommend starting range of motion of ankle as early as possible after suture removal preferably around two weeks and partial weight bearing around 4 weeks to prevent post-operative ankle stiffness. REFERENCES
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.