 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 6 Issue 3 - June 2018
Short term clinical outcome in mid shaft femur fractures using intramedullary nail
Tej Shah1, R N Shewale2*
1Resident, 2Professor and HOD, Department of Orthopedics, MGM Medical College, N-6, Cidco, Aurangabad-431003, Maharashtra, INDIA. Email: drtejshah@gmail.com
Abstract Background: Kuntscher was the first to introduce the concept of intramedullary nailing, later there were modifications in intramedullary nailing and for the first time Klemm and Schelmann, Grosse and Kempt and Russel Taylor developed proximal and distal fixation called intramedullary interlocking nail. Intramedullary nailing provide predictable restoration of femoral shaft alignment along with load sharing. Aim and Objective: To evaluate the status of intermedullary nail technique in unstable fracture femur with special emphasis on Time for radiological union ,Period of hospitalization, Early mobilization and Period of weight bearing after nailing. Methodology: 35 cases of fracture shaft femur were studied in our study, admitted to mahatma Gandhi medical college and Hospital between November 2014 and august 2016. All patients sustained a road traffic accident. Patient were analysed for short term outcome. Results and Discussion: 3 patients had ipsilateral tibial shaft fracture 1 patient had degloving injury over his right calf region, 1 patient had ipsilateral patella and proximal third tibial fracture. All patients were investigated according to the protocol and surgery performed between day 3 to day 7 after trauma, average duration was 6 days. Blood loss ranged from 150-300ml with a mean of 200ml. Key Words: mid shaft femur fractures, intramedullary nail.
INTRODUCTION Femur is the largest bone of the body and one of the principal load bearing bones in lower extremity. Fracture of the shaft of femur are major cause of morbidity and mortality in patients.1 Fracture of the shaft are the result of high energy trauma, which may be associated with multisystem injury and considerable soft tissue injury.2,3 Fractures of the shaft in elderly patients in due to osteoporosis and trivial trauma.4,5 Fractures of femur shaft may be predisposed due to pathological conditions of the femur.6 Urgent prompt reduction and rigid stable internal fixation is todays accepted mode of treatment, which will reduce the risk of pathophysiological complications as well as help to prevent permanent impairment of knee function by early mobilization. The method that is closely approaching this perfection is intramedullary interlocking nailing of femoral shaft fractures.1 Thus intramedullary interlocking nailing has been the gold standard for treatment of facture shaft of femur, and hence, early mobilization, minimal scarring of thigh muscles and early recovery of quadriceps and hamstring function. The physiological loading condition of femur by muscular and gravitational forces are also favourable for intramedullary fixation.
MATERIAL AND METHODS This is a prospective study of 35 cases of unstable fractures of the femur, treated at the Orthopaedic Department of MGM HOSPITAL OF HEALTH SCIENCES AURANGABAD with closed reamed intramedullary interlocking nail during November 2014 to October 2016. Inclusion Criteria: 1.Transverse, short oblique, communited, segmental fractures at the level of isthmus in adults. 2. Polytrauma patients where early mobilization is indicated 3.Failure to maintain reduction by conservative method. 4.Soft tissue interposition causing failure of reduction despite repeated manipulations. 5.Fracture involving upper or lower third of femur. 6.Fracture associated with head injury or paraplegia to aid constant turning of patient in bed. 7.Patients with age group of 18-65 years of either sex. Exclusion Criteria
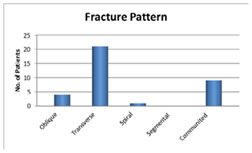
These cases of unstable fracture shaft femur were treated by femur interlocking nail, which is locally available and is based on AO design nail with proximal locking jig and two proximal and distal holes and one oblique proximal locking hole. The study was approved by the Ethical Committee of the Medical College All patients of unstable fracture shaft femur attended at the department of Orthopaedics were studied. A detailed history was taken of these patients and was explained about the investigations and study. Detailed history was taken about age, sex, occupation, mode of injury, past history and associated medical illness. Thorough clinical examination and general condition was assessed. X-rays are taken in 2 planes, AP and lateral including x-ray of ipsilateral hip and knee joints. All the fractures were classified according to AO classification. Preoperatively the length of nail was measured clinically and radiographically. Routine preoperative investigation assessment was done. Patients were operated under regional or general anesthesia after pre operative assessment. IV antibiotic was given 30 min before surgery. Oblique skin incision from the proximal tip of the greater trochanter taken and continued it proximally and poster-medially for 6-8 cm. Piriformis fossa was palpated. Entry point was made with curved pointed awl and medullary cavity was perforated at piriformis fossa, after confirming under image intensifier. A guide wire was passed through the proximal fragment and under C-arm control. The fracture was reduced and guide wire was passed in to the distal fragment. If reduction was not possible by closed means then fracture site was opened through lateral incision and open was reduction done. The position was confirmed under the image intensifier in AP and lateral plane and tip of guide wire was hammered in to the subchondral bone. Reaming was done. Reaming was performed in 0.5mm increments up to 1mm diameter larger than the chosen nail to make nail passage easier. Distal locking Was done with a free hand technique and using C-arm. Proximal locking was done with the help of proximal jig. Finally the whole length of the nail, reduction, proximal, and distal locking screws were checked under image intensifier. Open technique is necessary When close technique fails to reduce fracture fragments due to tissue interposition and acting muscular forces. For example in broken implant cases, Inability to pass guide wire in distal fragment and Cases operated more than 3 weeks after injury Postoperative care taken as follows Day 1: Early active flexion and extension are essential and encouraged .Day 2: Isometric and range of motion exercises begun Day 3: Gait training progressed from use of parallel bars to a walker or crutches, with weight bearing as determined by the stability of the intraoperatively. In patients with stable internal fixation, touchdown weight bearing of the affected extremity was allowed. In patients with comminuted fractures and with relatively unstable fixation, weight bearing is delayed until radiological evidence of fracture healing and a fracture brace may be needed. Day 8 to 10 : Suture removed. Prophylactic antibiotics were used in all patients. By 6 weeks, if X rays showed signs of union progression, increased weight bearing was allowed. By 12 weeks, with further evidence of radiological consolidation, full weight bearing was allowed. All the patients were followed up. With each follow up, clinical and radiological examinations were performed at 6 weeks,12 weeks,24 weeks and thereafter once in three months. RESULTS Functional results were graded based on the classification system for the results of treatment by Thoresen B.O., et al., (1985)7 Majority of patients were in the age group ranging from 18-60 years, youngest being 18, eldest being 60 years mean age being 33 years. Out of 35 patients 33 were male and 2 were females. In the present study all the patients had a history of Road Traffic Accident. Twenty seven cases were right sided and eight cases were left sided fracture shaft of femur. In the present study 21 were transverse fracture, 4 were oblique fracture, 1 was spiral and 9 were communited fractures. In our study three patient had associated tibial shaft fracture on the same side. One patient had ipsilateral degloving injury over the calf region. One patient had ipsilateral patella fracture and proximal third undisplaced tibial fracture. One patient had ipsilateral fracture humerus and 1 patient had fracture both bones of right forearm with lateral malleoli fracture. Average duration between trauma and surgery in our study was 6 days. Most common nail length was 400mm. Most common diameter nail used was 10mm and static locking done primarily in all patients. Partial weight bearing with crutches/walker was started on an average between postoperative day 2 to day 5. 9 patient with significant communition were advised delayed weight bearing. Mean time of union was 16 week in this study. Time to union ranged from 10 – 24 weeks. All patients had full range of motion at the hip and knee joint. Valgus angulation of 5 degrees was observed in 2 patients and varus. malalignment of 5 degrees was observed in 2 patient. No rotational deformities. patients had a shortening of 1.5 cms, 2 patient had shortening of 1cm, and 1 patient had shortening of 2cm. There were no cases of nonunion noted in our study. Superficial infection noted on 6th day in 2 patients that resolved with antibiotics. No instances of deep infectio were no instances of nail breakage in our study, nor any instance of breakage of locking bolts. 2 patients complained of sporadic knee pain persisting after fracture union. Table 1: Distribution of patients according to age
Figure 1: Distribution of patients according to sex.
Figure 2: Showing Fracture pattern
Table 2: Distribution of patients according to Associated Injuries
Table 3: Distribution of patients according to Postoperative mobilization
Table 4: Limb length discrepancy
Table 5: Assessment of functional results according to Thorensen Scoring
DISCUSSION Internal fixation of fractures of the femoral shaft has gained widespread acceptance as implants and technology have improved. The rationale for internal fixation is that it restores the anatomical alignment and allows early mobilization of the patient and limb. Studies have shown that the mean age of femoral fractures are between 20-35 years. In the study of Wiss et.al8 mean age was 29 years. Study of Thoresen (7) of 48 cases of femoral shaft fractures stated a mean age of 28 years. In most of the studies and in ours too the incidence was significantly higher in males. (33 males and 2 females). Mode of injury was road traffic accidents which was compatible to the other study in literature. In the study of Johnson et al9 right side was predominantly involved In the study of Wiss et al8 of communited fractures right side was predominantly involved. In our study right sided involvement was higher than the left. In the study of Thoresen et.al7 communited fractures were the commonest followed by the transverse and then the spiral pattern. In the study of Wiss et al8 communited fractures predominated. In our study the commonest fracture seen was the transverse variety followed by oblique and then the spiral type. Since femoral fractures most often are caused by high velocity injuries associated fractures are not uncommon. We had a ipsilateral tibial shaft fracture in 3 patients, ipsilateral proximal third tibial fracture in 1 patient, patella fracture in 1 patient, humerus fracture in 1 patient, lateral malleoli fracture 1 patient and fracture of both bones of forearm in 1 patient. Patients were operated between 3-7 days after trauma, average duration being 6 days. All cases were operated under spinal anaesthesia with pt supine and positioned on the fracture table. There was some difficulty in gaining access to the piriform fossa in a couple of obese pts in the supine position but adduction of the limb facilitated the procedure. Commonest length and the diameter of the nail used was 400mm and 10mm respectively followed by 380X10mm and 360X10mm nail. This in contrast to the western literature where most of the nails used is of a larger diameter (13 and 14 mm). In the study of Donald Wiss,8 average blood loss amounted to 470mlIn our study the average blood loss was 200 ml. Time to union of a fracture was defined as time from injury to full weight bearing and healing of the fracture characterized by bridging callus seen on two radiographs with different projections. In the study of Wiss et al (8) union was obtained at an average of 26 weeks. In the study of Thorensen et al7 of 48 cases of femoral fractures mean time to union was 16 weeks. In our study time to union ranged from 10 weeks to 24 weeks with an average of 16 weeks. Complications of nailing range from infections, malalignment, shortening, nonunion and failure of the implant. In the study of Wiss et al8 the infection rate after closed nailing was 0.9%, 11.5% lengthening and 3.5% shortening. In study of Thoresen et al7, 6.25% had varus malalignment, 2% had valgus malalignment, 2% had internal rotation and 4% had external rotation deformity. In the study of Christie et al11 0.8% had superficial infection, 1-6% had non union, 0.8%had external rotation and 1.6% had delayed union. In our study there were no cases of nonunion, valgus malalignment of 5 degrees in 2 patient with distal third fracture, varus malalignment of 5° in 2 patients, shortening of >l.5 cm was seen in 2 patient and 1cm in 2 patients and 2 cms in 1 patient. Superficial infection in 2 patient that resolved with antibiotics. There were no instances of deep infection. Sporadic pain in the knee persisting after union after the fracture seen in 4 patients. Out of 35 patients according to the Thorensen scoring system 31 patients had excellent results 4 patients had good results. Duration of surgery ranged from 80 min -160min with a mean of 90 min. Partial weight bearing was started at an average of 4 days and full weight bearing at mean of 13 weeks. Time to union ranged from 10-24 weeks with a mean of 16 weeks. We had our share of complications. Superficial infection was present in 2 patients that subsided with antibiotics. no cases of deep infection noted. No cases of non-union noted, valgus malalignment seen in 2 patient of 5 degrees. Varus mal alignment 5 degree seen in 2 patients. Shortening was noted in 4 patients, 2 had a shortening of 1 cm, 2 had shortening of 1.5 cm and 1 had shortening of 2 cms. All patients had a complete range of motion at the knee at union. Hip movements were full range in all patients. No cases of implant failure were noted. Out of 35 patients according to the Thorensen scoring system7 patients had excellent results 4 patients had good results
CONCLUSION Interlocking intramedullary nailing is a very effective and successful method of definitive primary treatment, in most types of fractures of the shaft of the femur. Closed nailing is preferred over open nailing, due to its faster rate of healing.
REFRENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.