 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 6 Issue 3 - June 2018
Clinical study clavicular fractures by surgical intervention
Prakash Channabasappa Wali1, Satish Shankar Nesari2*
1Associate Professor, 2Assistant Professor, Department of Orthopaedics, Belgavi Institute of Medical Sciences, Belgavi, Karnataka, INDIA. Email: pakwali@yahoo.com
Abstract Background: The most common fractures encountered in clinical orthopaedic practice are fractures involving the clavicles. The treatment of choice in comminuted or displaced fractures involving the clavicles was always conservative using Figure of 8 bandage. However, many of these fractures went in for non-union and some for gross malunion. Over time, for displaced fractures, internal fixation either percutaneously using steinman pin, K wire or TENS nail/ ORIF with plate and screws were used. This prospective study was conducted to evaluate the results of surgical intervention using a 3.5-mm reconstruction plate for the treatment of displaced clavicle fractures. Patients and Methods: Between January 2014 and November 2016, 25 patients with displaced clavicle fractures were treated with surgical intervention using 3.5 reconstruction plate. The prerequisites/indications for surgery included complete displacement and comminution classified following Allman's classification. Results: The mean time to union was 11 weeks (range 8–14 weeks). At the time of last follow-up i.e. 24 weeks, all the fractures were healed and the patients were advised to get back to their pre-injury activity. Conclusion: Surgical intervention is an effective and definitive treatment modality for displaced clavicle fractures, with few complications and early return of shoulder function. The procedure provides stable fixation, avoids risk to vital structures below the clavicle, and is associated with a low rate of implant-prominence problems. Key Words: Clavicle. Clavicle fractures. surgical intervention.
INTRODUCTION Clavicular fractures represent 2.6% to 5% of all fractures, and middle third fractures account for 69% to 82% of fractures of the clavicle. The junction of the outer and middle third is the thinnest part of the bone and is the only area not protected by or reinforced with muscle and ligamentous attachments. These anatomic features make it prone to fracture, particularly with a fall on the point of the shoulder, which results in an axial load to the clavicle. Optimal treatment of non-displaced or minimally displaced mid-shaft fracture is with a sling or figure‐of‐8 dressing; the nonunion rate is very low. However, when midshaft clavicular fractures are completely displaced or comminuted, and when they occur in elderly patients or females, the risk of non-union, cosmetic deformity, and poor outcome may be markedly higher. Thus, some surgeons propose surgical stabilization of a complex midshaft clavicular fracture with either plate‐and‐screw fixation or intramedullary devices1 More recent data, based on detailed classifcation of fractures, suggest that the incidence of non-union in displaced comminuted midshaft clavicular fractures in adults is between 10 and 15%. The literature favours rigid internal fixation with plates for symptomatic midclavicular nonunion2. However, the use of open-reduction in the treatment of fresh fractures is controversial, with wide geographic and institutional variations in the choice of treatment. More papers have been published on the complications of clavicle fractures and the treatment of non-union than on the primary operative treatment. Moderately displaced fractures of the mid-third of the clavicle can be treated non-operatively with satisfactory results. However, the results of non-operative treatment for severely displaced fractures (Allaman type 1b and 1c) in adults are poor.
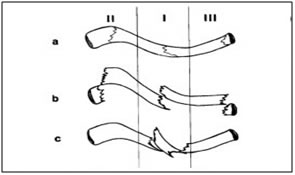
MATERIALS AND METHODS Since last 5 years, the standard treatment for displaced midclavicular fractures at our hospital has been operative. We found the Allman classification3 for midshaft fractures to be simple, and takes into account displacement and comminution. Between January 2014 and November 2016, a total of 25 patients were seen with acute non-pathologic mid-shaft fractures clavicle; 22 patients were Allman type 1b and 3 pts were Allman type 1c.All these patients were operated. Patients with multiple shoulder girdle injuries were not included. The fracture was caused by fall in 23 patients and by road-traffic accidents in 3 cases. All cases were operated upon within 3days of injury. The indications for operation included displacement of the bone ends by more than 100% of the diameter of the clavicle or the presence of fracture comminution. Allman's classification: Figure 1: Operative procedure: With the patient in a supine position, the operation was performed under general anesthesia or interscalene block. A longitudinal incision parallel to the long axis of the clavicle and centred above the fracture was made along the superior border of the bone. The fracture was plated with a 3.5 mm reconstruction plate. Comminuted fragments were reduced and held with cerclage wire. Interfragmentary screws were used as needed. The length of the plate was determined by the degree of comminution, and the aim was to restore clavicular length and to obtain purchase of at least 4 to 6 cortices on each side of the fracture. Bone grafting was not done primarily. Postoperatively, the limb was maintained in a sling for 4 weeks for patient comfort. No other support was used. The patients were seen at regular intervals until the final result of treatment was clear. Patients were questioned about pain, difficulty in lifting, pain with shoulder straps, pain on sleeping on affected side, local tenderness/numbness on palpation, impaired range of movement, impaired strength, signs of nerve compression, cosmetic abnormality, return to work, and overall patient satisfaction.
RESULTS All the 25patients were followed up for 6 months and data collected at earch visit. There were 22 men and 3 women, the average age being 37.3 years (range 22-65years). The right clavicle was fractured in 14 cases and the left in 11 cases. Cerclage wires were used in 2 cases and inter-fragmentary in 2 cases. No patient had neurovascular impairment or pulmonary injury attributable to the procedure. Pain subsided after 3 days post-operatively. The time to radiographic union was 8 weeks in 18 patients and 14 weeks in 7 patients. Clinically, 8 patients complained of mild soreness with weather and activity and 2 patients had impairment in terminal 20 degress of shoulder movement. These patients were elderly and diabetic, this did not handicap them from their daily activites. 18 pts after 8 weeks and 7 pts after 14 weeks with radiological union were advised to return back to their routine regular activites and were advised to abstain from heavy work. At 24 weeks they were advised to go back to the pre-injury activites.
DISCUSSION In this retrospective assessment we present the outcome of surgical intervention of fresh displaced mid-third clavicle fractures. Most orthopaedic surgeons prefer non-operative treatment for non-displaced middle-third fractures of the clavicle, using a sling or a figure 8 support. The optimal treatment modality for acute displaced middle-third fractures of the clavicle remains controversial, however4. Although most middle third clavicle fractures unite uneventfully, conservative treatment has been found to be associated with higher rates of non-union and patient dissatisfaction with the final result6. A prospective randomized controlled trial by the Canadian Orthopaedic Trauma Society compared plate and screw fixation with non-operative treatment for displaced middle third clavicle fractures5. The results showed that time to union was shorter in the operative group than in the non-operative group; moreover, surgical fixation of a displaced clavicle fracture resulted in improved functional outcome and lower rates of malunion and nonunion compared with nonsurgical treatment after a year of follow-up. Midshaft clavicle fractures get short shrift in medical texts. Craig, in classifying clavicle fractures, subdivided both medial and distal third clavicle fractures into five subtypes, but did not find it necessary to sub-classify mid-third clavicle fractures7 this despite the fact that midshaft fractures occur much more often than medial and distal fractures combined. We have found it useful to separate out the displaced and comminuted fractures when deciding management, and for years have been using a classification system of Allman. In this system, type 1b indicates a displaced midclavicular fracture, type 1c indicates comminuted or large butterfly fragment. The mechanism of injury was fall in 16 patients (64%) and road traffic accidents in 9 (36 %) patients. Robinson, studying 1000 adults, found 27% due to road traffic accidents8. The relatively high energy impact of motorcycle accidents probably accounts for the high percentage of open and comminuted fractures in this series. The many articles on the treatment of clavicular non union and malunion found on computerized literature searches, and referenced by Simpson and Jupiter9, suggest that the true incidence of nonunion is much higher. In Robinson's series8, the delayed union rate was 2.1% and the nonunion rate was 4.6% for type 2B1 fractures. For type 2B2, the delayed union rate was 6.3% and the nonunion rate was 9.4%. In Hill's series of displaced mid-third clavicle fractures6, 8/52 (15%) developed nonunion. White and Anson. Analyzed 112 adult clavicle shaft fractures retrospectively, and found 18 delayed unions and 9 nonunions10. When further subclassified, the nonunion rate was 13% in the high energy group. Our study found similar results as the study done by Robinson that the initial morphology of the fracture provides the best indication of the risk of delayed or nonunion, irrespective of the mechanism of injury. Plate fixation of fresh midclavicular fractures has been practiced for decades, yet very few clinical series have been published on the subject in the English literature11. To our knowledge, the largest is the series of 122 patients by PoigenfuÈ rst et al.12, 102 of which were midclavicular fractures. They found nine cases (7.3%) of superficial disturbances of wound healing, but no case of osteomyelitis or infected pseudarthrosis. In a study looking at closed treatment of displaced mid-third fractures of the clavicle, Hill et al.6 reviewed 52 out of 66 patients 38 months after injury, and found that 13 patients had pain requiring the use of medication, 20 patients had pain with shoulder straps, 23 patients had pain sleeping on the affected side, 20 patients had local tenderness on palpation, and 13 had notable cosmetic abnormality. Only 36 patients (69%) were satisfied with the result. Nonunion developed in eight fractures (15%). They recommended open reduction and internal fixation of severely displaced fractures of the middle third of the clavicle in adult patients. Stanley and Norris, while comparing the efficacy of figure-of-eight bandages versus a broad arm sling, stated that 33% of those over the age of 20 still had symptoms 3 months after fracture13. W.-J. Shen et al.14 in study of 251 patients stated early plate fixation may never become the treatment of choice for clavicular fractures, a knowledge of its outcome and complications is necessary to determine its relative merits. Figure 1: Figure 2:
Figure 3: Figure 1: Pre-operative X-ray with displaced butterfly fragment; Figure 2: Post-operative X-ray - treated with plate and screw with interfragmentary fixation of the butterfly fragment; Figure 3: Pre-operative X-ray with displaced butterfly fragment; Figure 4: Post-operative X-ray - treated with plate and screw with encirclage wire of the butterfly fragment The authors agree that clavicular fractures which are not severely displaced can be managed non-operatively. However, severely displaced and comminuted fractures behave differently from and should not be treated the same way as undisplaced or minimally displaced fractures. Closed reduction is rarely successful for displaced or comminuted clavicle fractures. The deforming pull of the sternocleidomastoid muscle is too great and the deformity recurs very shortly despite the use of supports such as the figure-of-eight bandage. At our hospital, acute surgical intervention of displaced clavicle fractures has been standard procedure for the past few years. The union rate has been 100%. Compared with non-operated patients pain relief is quicker, and even when malunion occurs, it is much less severe. Clinically, there is less problem with shoulder straps. Reconstruction plates can be contoured best to the complex three-dimensional anatomy of the clavicle. As with any tubular bone fracture, fixation of four or more cortices on each side is desirable. The plate should not be removed for at least one year, to avoid refracture.
REFERENCES
|
|

 Fgiure 4:
Fgiure 4: This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.