 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 6 Issue 3 - June 2018
Management of thromboangitis obliterans by ilizarov technique
Satish Shankar Nesari1, Prakash Channabasappa Wali2*
1Assistant Professor, 2Associate Professor, Department of Orthopaedics, Belgavi Institute of Medical Sciences, Belgavi, Karnataka, INDIA. Email: pakwali@yahoo.com
Abstract Background: ThromboAngitis Obliterans (TAO),also known as Beurger’s disease, is a progressive, inflammatory reaction in the arterial wall with involvement of neighboring vein and nerve, terminating in thrombosis of the artery. It is strongly associated with smoking. Clinically TAO presents as chronic ischemia (lower limb>upper limb). Materials and Method: A total of five patients diagnosed with TAO and treated using bone widening technique using Ilizarov external fixator were studied from March 2012 till September 2015. Relevant Investigations such as color Doppler and MR angiography was done whenever indicated. All the patients were followed up for >2yrs (mean=2years 9months). Patients were discharged after 10 days. Ilizarov apparatus removed after about 12 weeks. Results: In all patients, the severity of pain got reduced and dramatic improvement in claudication distance. Ischemic changes in skin improved. Conclusion: bone widening technique using Ilizarov method can be a good alternative in the treatment of Buerger’s disease. It is excellent and cost effective method. Key Words: thromboangitis obliterans, ilizarov technique.
INTRODUCTION Thrombo Angitis Obliterans (TAO),also known as Beurger’s disease, is a progressive, inflammatory reaction in the arterial wall with involvement of neighboring vein and nerve, terminating in thrombosis of the artery.1-3 TAO is more common in males. There may be some hormonal influence which suggests sex distribution3. TAO is a disease of male smokers. Though very rare, it is also seen in females4-6. Definite aetiology for the disease is unknown but it is strongly associated with smoking (primarily), also from use of smokeless tobacco. It is common in age group of 20-40 years. Histologically there are inflammatory changes in the walls of arteries and veins which may lead to thrombosis. Carl Friedlander in 1887 first named it as ‘arteritis obliterans’7. Three years later, in 1879,Felix von Winiwarter, came across a case of unusual obliteration of the arteries and veins of the leg in a 57 year old male patient, which he termed as endarteritis obliterans8. Leo Buerger, in 1908, gave first pathological description and called it ‘presenile spontaneous gangrene’9. As the acute histologic features in the arteries/veins were characterized by thrombosis and marked inflammatory response, he called it ThromboAngitis Obliterans. Clinically TAO presents as chronic ischemia (lower limb>upper limb). Usually, pain is the presenting complaint (claudication /rest pain). Associated features like chronic ulcers/gangrene may be present. History of tobacco use (smoking/smokeless tobacco) is present. Though there is no permanent cure as of now, cessation of tobacco in any form should be the first step/most effective step10,11 in treatment and results in disease quiescence but doesn’t reverse the disease. Various medical (Platelet inhibitors, vasodilators, anti-coagulants, thrombolytic therapy, clofibrate etc.), surgical (thrombolytic therapy, bypass grafts, lumbar sympathectomy, omental transfer etc.) and other modalities (spinal cord stimulation, therapeutic angiogenesis) have been tried with limited success. As the disease progresses, Amputations may eventually be required. Periosteal stripping12, cell therapy, vascular gene therapy13, osteotrepanation14 are newer modalities in treatment. GA Ilizarov has studied effect of tension stress on genesis and growth of tissues in canine tibiae and found that corticotomy and distraction of fragments increased blood supply to the limb and led to osteogenesis and neo-histogenesis15,16. Buerger’s disease can be effectively managed using the principles of distraction osteogenesis to promote angiogenesis. Ilizarov’s method of distraction osteogenesis increases vascularity of the ischemic limb, thereby preventing subsequent amputations at higher level. However it needs considerable skill and expertise and has a long learning curve. Although distraction osteogenesis is shown to promote angiogenesis, using this technique as a treatment modality has been reported by only a few. We report here our experience in treating three patients diagnosed to have Buerger’s disease (Thromboangitis Obliterans) using bone widening technique using Ilizarov external fixation technique.
MATERIALS AND METHODS A total of five patients diagnosed with TAO and treated using bone widening technique using Ilizarov external fixator were studied from March 2012 till September 2015. History of heavy smoking(20-40 beedis/day, for >25 yrs) since early age was present in all cases. All patients had severe rest pain. All patients had grade IV ischemia as per Rutherford classification and stage IV disease as per Leriche-fontaine classification. Other possible causes of ischemia such as atherosclerosis, Raynaud’s phenomenon were excluded before the diagnosis of TAO was made. Relevant Investigations such as color Doppler and MR angiography was done whenever indicated. All patients had received some or the other pharmacological treatment with limited success. Mean age was 43 yrs. Four patients had lower limb involvement(chronic ischemic features with non healing ulcer). In three patients, popliteal, posterior tibial, dorsalis pedis were not palpable, though femoral arterial pulsations were palpable. Peripheral capillary oxygen saturation by pulse oximetery was not recordable. Three out of five patients had gangrene of great toe for which amputation (guillotine method) of great toe was done followed by bone widening by Ilizarov technique. One patient had involvement of upper limb in addition with chronic ischaemic features in left hand and gangrene of left index finger/thumb. Radial/ulnar artery pulsations were not palpable. He had segmental narrowing and occlusion of brachial artery, ulnar and radial arteries which was operated by vascular surgeon before presenting to us. After removal of block, there was some improvement in pain but later as the symptoms worsened, the patient was advised for above elbow amputation. Ilizarov technique was tried prior to amputation. As there was considerable improvement in signs/symptoms, amputation was avoided. Post-operatively, weight bearing was allowed soon after operation, patient is allowed to mobilize soon after the pain decreased. Patient is able to walk about 7 days post surgery. All the patients were followed up for >2yrs (mean=2years 9months). In the last follow-up, all the patients are able to walk for >1.5 km and they resumed to their duties. Technique: Corticotomy was performed on the antero-medial surface of tibia. Percutaneous multiple small vertical incisions were taken. The longitudinal osteotomy was made on the antero-medial surface of tibia using 5mm osteotomes. This results in small fragment of tibia (about 12-15cm long), in the postero-medial area which is distracted apart horizontally using crossed plain wires. Osteotomy fragment was fixed with cross wire technique. Post-op care: Regular dressings were done to prevent pin tract infection. Physiotherapy was advised post operatively. After a period of 7days distraction was started. Rate of distraction being 0.25mm, 4 times/day. Total distraction was 2-2.5cms.consolidation period was about 10 weeks. External fixator time was about 12 weeks. Post-op radiographs were taken every 6 weeks till frame is removed. Patient is able to walk bearing full weight in few days after surgery. Patients were discharged after 10 days. Ilizarov apparatus removed after about 12weeks. RESULTS Improvement in symptoms was gradual, pain relief seen after 2 weeks following treatment. In all patients, the severity of pain got reduced and dramatic improvement in claudication distance. Ischemic changes in skin improved. By the time fixator was removed, ulcer showed signs of healing. Oxygen saturation measured using pulse oxymeter was>95% at the time of fixator removal. All the patients now are able to walk >1.5 km with minimal/no pain. All patients resumed to their duties/jobs.
Figure 1 Figure 2 Figure 3 Figure 4
Figure 5 Figure 6 Figure 7
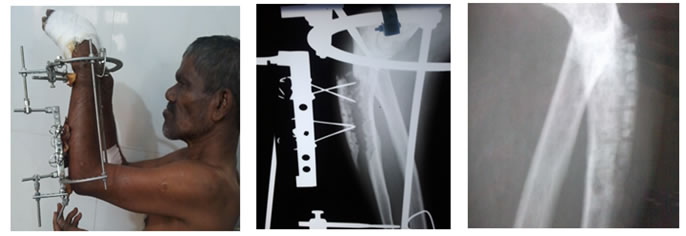
Figure 8 Figure 1: Full weight bearing-five days after surgery; Figure 2: Osteotomy fragment fixed using crossed wire tecnique and ilizarov fixator; igure 3: Healed osteotomy site post removal (12 weeks) of ilizarov fixator; Figure 4: Upper limb tao; Figure 5: Upper limb tao operated using ilizarov fixator; Figure 6: Osteotomy fragment fixed using crossed wire tecnique and ilizarov fixator; Figure 7: Healed osteotomy site post removal(12 weeks) of ilizarov fixator; Figure 8: Post ilizarov picture showing pulse oxymetry parameters. DISCUSSION Thrombo Angitis Obliterans (TAO), also known as Beurger’s disease/pre-senile gangrene, is a progressive, segmental, non-atherosclerotic, inflammatory, vaso-occlusive disease (thrombosis) of small/medium sized arteries and/or thrombophlebitis of superficial or deep veins and Raynaud’s syndrome.1-2,17 The disease is more prevalent in middle east and asia18.Though definite aetiology is unknown the possible aetiologies include/attributed to use of tobacco, genetic predisposition, autonomic overactivity, autoimmune aetiology3. Pain is typical of intermittent claudication which progresses to rest pain. Gradually, postural color changes appear, followed by trophic changes and eventually ulceration and gangrene of one or more digit; finally of the entire foot and hand requiring amputation. As the disease progresses pain becomes intense and may be even present at rest (rest pain). Rest pain is so intense that patient cannot sleep, some amelioration may be achieved by placing the affected limb in dependant position 3,17. Signs suggestive of chronic tissue ischaemia are present. The most frequent finding is absence of posterior tibial and dorsalis pedis pulses in the feet. Absence of posterior tibial pulse when bilateral is highly suggestive of the disease. In the upper extremity, the radial pulse may be absent and when bilateral is suggestive of disease3. Recurrent superficial thrombophlebitis is a characteristic feature of the disease18. Migratory superficial phlebitis may be present in upto16% of patients, thus indicating a systemic inflammatory response17. Some of the characteristic angiographic findings include - disease confinement to distal circulation, the occlusions are segmental and show skip lesions with extensive collateralization (corkscrew collaterals)17. Conservative treatment comprises cessation of smoking/tobacco use. But only 43-70% of cases manage to give up smoking19. Vasodilators, anti-coagulants, dextran, phenylbutazone, steroids, prostaglandin therapy have been tried with questionable vaue3. Role of sympathectomy is doubtful3,17-18 and has got specific role in alleviating pain. About 50% of patients are significantly benefitted from sympathectomy3. Though sympathectomy is shown to promote ulcer healing and provides short term pain relief in some patients with Buerger’s disease, no long term benefits has been confirmed20. Re-vascularising options are limited17. Arterial reconstruction is difficult because of the distal nature of the disease, amputation is the only way out when gangrene develops3. Distraction osteogenesis is a surgical technique used to reconstruct skeletal deformities and lengthen the bones. A corticotomy is used to fracture the bone into two segments and the two segments are gradually moved apart during which new bone forms in the gap21-22. Intact medullary blood supply, preservation of soft tissue envelope, mainly the periosteum and stability of fixator are the most important factors for success of bone distraction23-24. Distraction rate must be gradual to achieve optimal results. Too slow distraction rate would result in early bone consolidation whereas rapid distraction may result in fibrous union 25. Treatment of TAO in our study is based on principle of law of tension stress by prof. Ilizarov which states that ‘when living tissues are subjected to uniform planar distraction forces after atraumatic corticotomy in the presence of intact functions new tissues (bone, muscle, fascia, nerve, vessels, skin) regenereate in the limb’ neovascularisation leads to increase in collateral circulation and blood supply is increased up to 1.5-2.7times. Bone widening by Ilizarov method can be considered as best method in failed cases treated by other modality, in the management of TAO. Factors responsible for neo-histogenesis include atraumatic corticotomy, stability of fixation, intact function/vascularity, rate of distraction. Ilizarov technique increases blood supply to bones/muscles, the operative time is <1hr, the blood loss can be minimized to <20ml,the technique is cost effective and hospitalization needed is <10 days. The main disadvantage is pin tract infection which can be effectively managed by regular proper dressings. Shevstov et al.26 studied 265 patients with TAO treated by distraction osteogenesis and followed up for 3years, results were good in 89 % (236) patients. In a study by JJ patwa et al.27 in which 60 patients were treated with Ilizarov technique with a mean follow-up of 5.4yrs, there was significant improvement in 53 patients in terms of rest pain, claudication distance, ulcer healing, decrease in higher amputation. However 18 patients had pin tract infection and 2 fractures. 2 patients had amputation. Chaudhary et al.28 reported 30 patients with TAO managed using bone widening technique and followed up for >2 years and found that >90% had good results but amputation in 3 patients and infection in 2 cases. Fokin et al.29 studied 125 patients with TAO treated using distraction osteogenesis with an average follow-up of 21.6 months, 94.2% of the patients had good results. However 16 cases had local infection and 2 had fracture as a complication. Kulkarni et al.30 treated 30 patients with Buerger’s disease using Ilizarov fixator with a mean follow-up of 4.5yrs and found 83.3% had good results, whereas in 4 patients amputations were done and 2 had infection.
CONCLUSION We conclude that bone widening technique using Ilizarov method can be a good alternative in the treatment of Buerger’s disease. It is excellent and cost effective method. It can avoid amputations at higher level and provides relief of symptoms, may halt/retard disease progression when accompanied by cessation of tobacco use in any form.
REFERENCES
|
|

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.