 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 7 Issue 1 - July 2018
Shaft Humerus Fractures Treated with Interlocking Nails Vs Dynamic Compression Plate - A Comparative Study
Mohd Abdul Naser1, Ritesh Pathak2*, Athar Ahmad3
1Assistant Professor, 2Associate Professor, 3Associate Professor, Department of Orthopedics, IIMSR Medical College, Badnapur, Jalna, Maharashtra, INDIA Email: driteshpathak@gmail.com
Abstract Background: Fractures of shaft humerus are very common. This study was conducted to assess the outcome of this fracture by two most common mode of treatment that is open reduction internal fixation with DCP and Close Humerus interlocking nail. Methods: Shaft humerus fractures account for approximately 2 to 3 % of all fractures and are commonly encountered in clinical practice. Many can be managed conservatively and those that are operated can be treated by either plating or nailing techniques. Results: This study was done to compare the two commonly performed surgical techniques. 60 patients who were admitted with fracture shaft of humerus and given operative treatment were studied for functional outcome, radiological outcome and complications of the procedure. 30 of these patients were treated with ORIF with Dynamic Compression plates and the remaining 30 were treated with CRIF with IMIL nails Follow up showed a statistically significant difference in the operative time, operative blood loss and hospital stay post-surgery all in favour of the IMIL nail group. Functional outcome in both the groups was comparable except for a statistically significant increase in the incidence of shoulder related complications, and increased risk of implant failure in the IMIL nail group. No significant difference was seen in the radiological outcome between the groups. Conclusion: We concluded both humerus interlocking nail & dynamic compression plating has their own advantages & disadvantages and so can be used with equal preference. Key Word: Shaft Humerus Fractures, Interlocking Nails, Dynamic Compression Plate
INTRODUCTION Fracure humerus can be managed conservatively with casts like hanging casts and functional braces.1,2 Results of conservative treatment are well accepted as mal union is well tolerated by patients3,4 Operative treatment is mostly indicated in compound fractures of humerus, polytrauma, pathological fractures, floating elbow, communited fractures and fractures associated with vascular injury.5,6 Most common technique for internal fixation of fracures are plating and intramedullary nailing. Both procedures have their own advantages and disadvantages. Plating demands extensive soft tissue dissection and periosteal stripping with a long operating time but can provide a more stable fixation, can reduce chances of malunion and it allows for direct visualization of the radial nerve7 Intramedullary nailing on the other hand offers lesser operating time and minimal soft tissue damage at the cost of shoulder related complications, iatrogenic radial nerve injury and incomplete reduction of the fracture.6,7 Thus this study was done to compare the functional results, radiological outcomes and complications of two methods available to fix humerus shaft fractures; i.e. ORIF with Dynamic compression plates and CRIF with Intramedullarynails. MATERIALS AND METHODSA comparative study was carried out at Noor Hospital of IIMSR Medical College, Badnapur, Jalna, Maharashtra during the period of May 2014 to May 2017. All patients who were included in the study were thoroughly examined after history taking and an informed consent was taken. The patients were randomly assigned into either the plating or the nailing group. 30 of the patients underwent ORIF with Dynamic compression plates and 30 underwent CRIF with intramedullary interlocking nails. All patients aged more than 17 years (with humerusphyses closed), with shaft humerus fractures less than 7 days old requiring surgery were included in the study. Patients aged less than 17 years, those with pathological fractures, those with neurovascular deficits, patients medically unfit for surgery and compound fractures of Grade 3 were excluded from the study. The patients in the plating group were operated with either the posterior approach or antero-lateral approach. The fracture was fixed with a 4.5 mm Dynamic Compression Plate. A minimum of 6 cortices were purchased on either side of the fracture with 4.5 mm cortical screws. The patients in the nailing group were operated with anterograde nailing using ahumerus intramedullary nail. After taking an appropriate incision and entering the bone with an awl, serial medullary reaming was done and the nail with largest possible diameter was inserted over a guide wire. Before inserting the proximal locking bolts, the soft tissues were meticulously dissected and any overlying neurovascular bundles were retracted. The nail was then locked proximally and distally with cortical bolts under fluoroscopic guidance. Postoperative radiographs were taken to confirm adequate reduction. The patients were given injectable antibiotics and analgesics for 2 days and then switched onto oral medication. The patients were kept in an arm sling following surgery and encouraged to perform pendulum exercises and passive followed by active range of movements of the elbow from the 1st post- operative day. The patients were discharged on 3rdpostop day once they were pain free and adequately mobilized. The patients were followed up in the outpatient department at 2 weeks, 3 months, 5 months, 10 month and at 1 year. The patients were examined clinically at each visit to look for signs of surgical wound infection, range of movements at elbow and shoulder and any other complications. At every visit a plain radiograph was taken and signs of hardware failure, screw back out and signs of union were looked for. The fracture was said to have united if bridging callus was visible on at least 2 orthogonal view radiographs. The normal union time was taken as 4 months, delayed union as that occurring between 4 to 6 months and non-union as no signs of fracture union beyond 6 months. The functional status of each patient was assessed at the end of 1 year using the ASES score (American Shoulder and Elbow Surgeons score). This scoring gives a maximum of 4 points to 13 different activities of daily living that are required by patients. The maximum score given is 52. Functional results were also graded by the criteria of Rommens et al. Shoulder and elbow functions were graded excellent, moderate or poor depending upon the loss of range of motion in any direction, subjective complaints like pain was also taken into account. RESULTSTable 1: Post-operative shoulder movements
In our study, 30 patients underwent internal fixation with interlocking nails, and 30 with dynamic compression plates (As shown in Table 1). Table 2: Comparison of pre-operative evaluation between Nailing and Plating group
No statistically significant difference was noted between the two groups when the baseline demographics were compared making the two groups comparable. The perioperative parameters were compared and the results tabulated (As shown in Table 2). Table 3: Comparison between intra-operative and post-operative analysis
It was seen from Table 3 that the statistically significant difference was noted in the average duration of surgery, average blood loss and average duration of hospital stay after surgery (p<0.05) between the two groups, all in favour of the nailing group. The nailing group had 2 and plating group had 4 patients with surgical wound superficial infection, which were all treated by appropriate antibiotics and debridement. No deep infections or osteomyelitis cases were reported in either group. The functional and radiological outcome and complications that were recorded at each follow up were tabulated and compared. Table 4: Post-operative results for Nailing and Plating group
It was seen from Table 4 that most patients in both the groups had union on x- rays before the 16thweek of follow up after surgery. The average ASES scores were comparable in both the groups at the end of 1 year following surgery although the nailing group showed an increased incidence of shoulder stiffness which was statistically significant (p<0.05). The Rommens scores at 1 year follow up showed an excellent result in both the groups in a majority of the patients, 78% in nailing group and 77% in plating group. The most common complication observed in the nailing group was shoulder stiffness, which was treated with physiotherapy and gradual range of movement exercises. All patients recovered and had a good functional range of movements at shoulder at the end of 1 year following surgery. We recorded 4 cases of post-operative radial nerve palsy which were all neuropraxias. 2 were seen in the nailing group and were attributed to manipulation of fracture during surgery. 2 cases were seen in the plating group and were attributed to irritation by hardware. All the patients recovered completely within 3 months with splinting and physiotherapy. No cases of axillary nerve injury were recorded in either group.
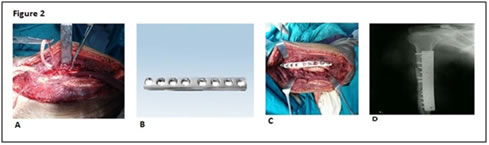
Legend Figure 1A: Pre Operative X-Ray Of Fracture Shaft Humerus; Figure 1B: Post Operative X-Ray of Humerus Interlocking Nail. Figure 2A: Posterior Approach; Figure 2B: Dynamic Compression Plate; Figure 2C: Fracture Fixed With DCP; Figure 2D: Post Operative X-Ray. DISCUSSION Increasing trend towards operative management is being seen nowadays to allow patients an early return to their daily activities and occupation. Ikpeme JO et al.8 CRIF with intramedullary nails was known to be less invasive and had a lower incidence of intraoperative radial nerve damage. Thus it has arisen as a viable option for treating humerus shaft fractures. Open reduction with plating shaft humerus fractures, blood loss and risk of damaging radial nerve during surgery stimulated many to look for an alternative mode of treatment. An extensive meta-analysis was done to compare the results of intramedullary nailing and plating techniques in the treatment of these fractures by Canavese F et al.9 They concluded that no significant difference exists between the two techniques except for an increased incidence of shoulder related complications in the nailing group. Suh JT et al. 10 also performed ameta-analysis to compare these two implants in treating shaft humerus fractures and found that nailing had an increased incidence of shoulder related complications, fracture comminution during surgery, higher rate of implant failure and resurgery, with no significant difference seen in time to union or radial nerve injuries. Similar results were also reflected in our study, where we recorded no significant difference in radiological outcome and time to union between the two groups. We observed that the functional outcome was also similar except for a statistically significant increase in the incidence of shoulder stiffness following surgery in the nailing group. A higher rate of implant failure was also noted in the nailing group.
CONCLUSION Based on our operative results on follow up of cases, we conclude that both humerus interlocking nail & dynamic compression plating has their own advantages and disadvantages and so can be used with equal preference.
REFERENCES
|
|

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.