 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 7 Issue 2 - August 2018
Functional outcome of total knee arthroplasty among patients having osteoarthritis
Milind Kulkarni1, Shekhar Malve2*, Arpit Sekri3, Ruta Kulkarni3, Madhura Kulkarni3, Sujay Kulkarni4
1Professor, 2Assistant Professor, 3Associate Professor, 4Resident, Department of Orthopedics, PGI Swasthiyog Pratishthan, Dr. G.S. Kulkarni Hospital, Miraj, Maharashtra, INDIA. Email: shekhardoc82@gmail.com
Abstract Background: Primary osteoarthritis is more common in weight bearing joints. More than 85% of individuals older than 65 years of age have radiographically visible osteoarthritis. Objective: To assess the post-operative functional results in the replaced knee. Methodology: Experimental study conducted by involving 25 patients with 30 knee sites having diagnosed osteoarthritis. Results: Majority of knee sites i.e. 66.7% were unilateral and 33.3% were bilateral. Out of 30 sites operated 17 i.e. 56.7% were female knees and 13 i.e. 43.3% were male knees. Mean age of study population was 63.4 years. 64% could walk more than 10 blocks. 24 (80%) knee joints out of 30 achieved movements range upto 90 to 100 degrees postoperatively. Conclusion: Relief of pain is predictable and often total. Walking ability of all the patients improved significantly with good stability of knee joint. Key Words: Outcome, total knee arthroplasty, osteoarthritis.
INTRODUCTION Osteoarthritis is the result of mechanical and biological events that destabilize the normal processes of degradation and synthesis of articular cartilage, chondrocytes, extracellular matrix and subchondral bone. Osteoarthritis can be primary or secondary. Primary osteoarthritis generally is a degenerative arthritis of unknown origin that may be active to some extent in several joints and rarely occurs before the age of 35 years.1 Secondary osteoarthritis usually is monoarticular, in which the reaction of a joint to some condition has produced articular incongruity. Mechanical derangement, pyogenic infection, congenital anomaly, physeal separation, ligamentous instability and intraarticular fractures are among the common causes of secondary osteoarthritis.2 The prognosis is better for primary type than for secondary type. The end stage of the types is the same, but the progression of primary osteoarthritis is usually slower and less relentless3.Primary osteoarthritis is more common in weight bearing joints. More than 85% of individuals older than 65 years of age have radio graphically visible osteoarthritis.4,5 For an individual of more than 50 years of age with moderate to severe osteoarthritis who is ready to forego high impact activities, total knee arthroplasty is an excellent option. Postoperatively, the patients should avoid impact loading such as running jumping, skiing. However, bicycling, walking and swimming are allowed without restriction. More recent studies have reported similar results for both younger and older patients without premature implant wear, loosening and osteolysis as reported earlier. Patient selection is crucial. Laborers and very active individuals are not candidates for this procedure unless they are willing to modify their activity levels. Total knee arthroplasty is an excellent treatment modality in severe tri-compartmental osteoarthritis of knee in older individuals with limited physical activity and when all other treatment modalities have been exhausted 6-17. So with background we wanted to know the functional outcome of total knee arthroplasty conducted on indicated patients of osteoarthritis in our hospital at Miraj city.
MATERIAL AND METHODS A total of 30 total knee arthroplasties performed at this institute were selected for study and were prospectively followed from September 2013 to October 2015. All selected cases were operated for primary osteoarthritis of knee Inclusion Criteria
Exclusion Criteria
Post-operatively all the knees were evaluated with anteroposterior and lateral radiographs taken immediately postoperatively and also at each follow-up visit. Following points were considered in evaluation:
RESULTS Table 1: Distribution according to side, gender and number of knees involved
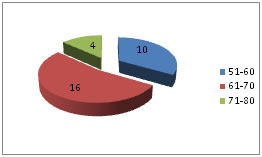
Number of subjects were 25 and number of knees operated were 30. Majority of knee sites i.e. 66.7% were unilateral and 33.3% were bilateral. Out of 30 sites operated 17 i.e. 56.7% were female knees and 13 i.e. 43.3% were male knees. Figure 1: Distribution of knees according to age group Out of 30 operated knees, 16 were from age group of 61-70 years followed by 10 from 51-60 years. Mean age of study population was 63.4 years.
Table 2: Subjective evaluation of operated patients
Subjective evaluation of patients stated that 92% were completely satisfied and 4% were moderately satisfied.
Table 3: Objective evaluation of operated patients with reference to function
Functional evaluation proved that more number of patients could walk up to 5-10 blocks (28%) or even more than 10 blocks (64%). One patient could walk unlimited after the operative procedure
Table 4: Objective evaluation of operated patients with reference to range of motion
24 (80%) knee joints out of 30 achieved movements range upto 90 to 100 degrees postoperatively.
DISCUSSION Taking into account the dramatic relief of pain and restoration of function, after total knee arthroplasty, it is clearly the optimum form of major reconstructive surgery for the arthritic knee in the middle aged and the elderly unless contraindicated.6-17 A total of 25 patients with 30 knees were selected from the outdoor clinic. A preoperative examination and assessment proforma was made and used in all cases. All had tri-compartmental osteoarthritis of knee. The number of patients with osteoarthritis is more than all other causes of arthritis of the knee joint. This correlates well with findings of Insall and associates8 in whose series 336 had osteoarthritis and 125 had rheumatoid arthritis. For the same reason we have chosen 30 cases of osteoarthritis for the present study. Ranawat et al10 undertook a study to evaluate the results of total knee arthroplasty in patients younger than 55 years. Majority of the 93 knees were from rheumatoid arthritis group (RA 76, OA 17). The results indicated a cumulative survivorship rate of 96% at the end of 10years. These are comparable to older patients and better than total hip arthroplasty in younger patients. In our series, 8 knees were less than 60 years of age and results at a short follow up were comparable with patients in older age group. In our series, pain not amenable to drugs was a dominating feature, all the 30 patients walked less than 10 blocks preoperatively and were further restricted from walking by pain, flexion deformity (10to 25 degrees) and instability (5 to 15 degrees) with restricted or painful range of motion. At the last follow up, 29 patients were virtually pain free, 1 had mild pain. Pain in the case with mild pain was well controlled with physiotherapy and analgesics. Postoperatively, all the patients could walk more than 5 blocks, there was evidence of flexion deformity in 1 knee and out of 30 operated knees, only one had mild valgus alignment of the lower limb attributed to radical soft tissue release at the of surgery. There was no varus deformity. Thus we could provide a stable, pain free and functional knee to each of our patients. The patients were explained before surgery the modifications they would have to do and the alterations in their lifestyle eg not to sit cross-legged, use dining chair, use western style toilet. All the patients preferred changes in life style than suffer from disability and pain and were well adapted to it. In series of 354 osteoarthritic knees treated by primary cemented kinemax total knee prosthesis over the end of 5 years results reported by D. L. Back, S. R.. Cannon, A Hilton18 are as follows: The knee rating score improved from 28 preoperatively to 96 postoperatively. In another series of 5-8 years follow up of cemented kinemax total knee replacement, Ewald reported improvement of knee score from 36 preoperatively to 96 postoperatively. Another study reported by G.S.Gill and AB.Joshi19 of 8-10 years follow up of 404 kinematic condylar knees showed following results:
Mean knee score improved from 36 preoperatively to 94 postoperatively. Figure 1: PREOP Figure 2: POST OP
CONCLUSION Following conclusions can be drawn after the results obtained: 1. Relief of pain is predictable and often total. 2. Walking ability of all the patients improved significantly. 3. Good stability of knee joint was obtained. 4. Roentgen graphic study upto the last follow up did not show shift of components, loosening, ectopic bone formation
REFERENCES
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||


 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.