 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 7 Issue 2 - August 2018
Evaluation of outcome of medial opening wedge high tibial osteotomy with an external ring fixator for medial compartment osteoarthritis of knee with varus deformity
Ansari Abdullah1, Mohd. Abdul Naser2*, Anil Dhule3
1Assistant Professor, 3Associate Professor, Department of Orthopediatics, Government Medical College, Aurangabad, Maharashtra, INDIA. 2Assistant Professor, Department of Orthopediatics, IIMSR Medical College, Badnapur, Jalna, Maharashtra, INDIA. Email: amanhospital@gmail.com
Abstract Background: There are very few studies regarding the clinical outcome of high tibial medial opening wedge osteotomy in osteoarthritis of knee. The aim of the study is, To evaluate the outcome of medial opening wedge high tibial osteotomy for medial compartment osteoarthritis of knee, To evaluate the deformity correction by X-ray, CT Scanogram and assess the relief of symptoms of osteoarthritis, function, pain and patient satisfaction using Knee Society scoring system. Methods: We prospectively followed 50 consecutive patients with medial compartment osteoarthritis of knee joint requiring surgery. In our study the patient data, the knee joint pain, knee joint deformity, knee joint mechanical axis, the knee society score were recorded pre-operatively and post-operatively. Pain was analysed using visual analogue scale both pre and post operatively on the visual analogue scale for pain. The varus deformity in these patients were graded as mild (0-5 degree), moderate (5-10 degree) and severe (7-10 degree. The Mean mechanical axis in the pre and post operative group were statistically analysed with the help of student T test. Results: A Total of 50 patients were included in the study. 33 patients (66%) had moderate deformity and 17 patients (34%) had severe deformity pre-opereratively. Pain was analysed using visual analogue scale both pre and post operatively on the visual analogue scale for pain. Pre-operatively majority of the patient had score of 8 (40%), followed by 7 (30%) and 6 (20%) and 9 (10%). Post operatively majority of the patient had a score of 1 (25%) followed by a score of 2 (15%) and then score of 3 (10%). The pain score when compared on student T test was found to be decrease by 5 points after surgery. The Mean Knee Society Score pre-operatively was found to be 33.6 which improved post-operatively to a mean score of 84.02. Conclusion: We concluded that significant improvement in the knee joint pain due to osteoarthritis was achieved post-operatively. The mechanical axis correction was significant. There was significant improvement in the knee society score following high tibial wedge osteotomy in medial compartment osteoarthritis of knee. It is a safe and efficacious technique and offers major advantage of outpatient surgery. The complications were too minimal like pin tract infections and were adequately treated. Key Words: Osteoarthritis, Anteroposterior, Total Knee Arthroplasty, Diabetes mellitus, Chronic Obstructive Pulmonary Disease.
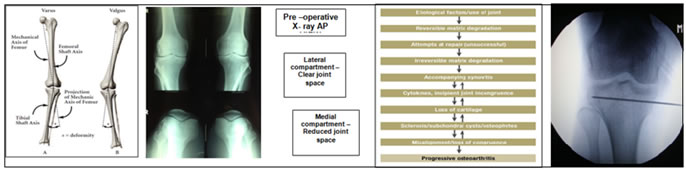
Knee osteoarthritis ranks among the most common disabling and costly health condition in adults and its prevalence is projected to increase sharply over the next decades1. Medial compartment osteoarthritis is associated with genu varum, medial joint space narrowing, medial joint laxity, and quadriceps weakness, as well as sclerosis and attrition of subchondral bone2.
MATERIALS AND METHODS A total 50 patients with medial compartment osteoarthritis of knee presented to Government Medical College and Hospital, Aurangabad, Maharashtra between May 2012 and May 2014 were included for the study. After appropriate work up and informed consent all the patients diagnosed to have medial compartment osteoarthritis of knee who fulfil the inclusion criteria underwent medial opening wedge high tibial osteotomy with external ring fixator followed by application of proximal tibial plate. Inclusion Criteria: Patients less than 60 yrs, Flexion of at least 90 degree, fixed flexion deformity of not more than 15 degree, Varus deformity of less than 20 degree, No internal derangement of knee Exclusion Criteria: Bicompartmental OA, Symptomatic patellofemoral compartment, OA, Valgus knees, Femoral deformity, Rheumatoid arthritis. Implants Used: External fixators, olive wires, wire tensioner, telescoping rod, centric and eccentric screws, proximal tibia plate. Patients were counseled preoperatively about the procedure and alternative option of TKR and informed consent was obtained. Radiographic assessment, Preoperatively patients had weight-bearing anteroposterior (AP) and lateral radiographs centered on the knee, and Standard AP and lateral radiographs of the tibia and fibula and skyline view to assess the patello-femoral arthritis. Correction planning was performed using long leg standing AP radiographs. Preoperative radiographic OA grade was recorded using The Ahlback11 classification. According to Ahlbäck system knee joint osteoarthritis is classified as- Grade 1 - joint space narrowing (less than 3 mm), Grade 2: Joint space obliteration, Grade 3: Minor bone attrition (0-5 mm), Grade 4: Moderate bone attrition (5-10 mm), Grade 5: Severe bone attrition (more than 10 mm). Routine blood investigations, blood grouping and typing, urine routine, blood sugar, serum urea, creatinine, serum bilirubin, HbsAg, HIV, chest x-ray, ECG, were done in all cases. Necessary and adequate treatment was given for those associated with medical problems such as anaemia, diabetes, hypertension, ischemic heart disease, hypothyroidism, chronic obstructive pulmonary disease, asthma, etc were evaluated and treated before taking them to surgery. Surgical Procedure: Patient positioned supine on the operation table with operative limb in neutral position. The operation was performed under general or spinal anaesthesia.1.5 gm of prophylactic Cefuroxime was given intravenously. A pneumatic thigh tourniquet was applied and inflated only when required..The frame was applied using the ‘‘rings first’’ method. The leg was rotated so that the patella was facing forward. Using fluoroscopic imaging, a smooth 1.8-mm illizarov wire was advanced across the proximal tibial metaphysis from lateral to medial in the coronal plane, perpendicular to the proximal tibial mechanical axis. The wire was placed at least 15-mm distal to the lateral tibiaplateau in order to avoid penetrating the joint capsule. The proximal ring was centred on the leg and the wire tensioned. The ring was held perpendicular to the mechanical axis of the tibia in the sagittal plane. A second wire was placed anterior to the fibula head exiting the anteromedial part of the tibia. The wire was advanced in a normal fashion, whilst watching the foot for motion. Once the wire tip had crossed through the leg and was tenting the skin, the drill was removed and the wire tapped through. A third wire was placed, from posteromedial to the anterolateral aspect of proximal tibia. All wires were tensioned. The distal ring was fixed with 2 steinman pins. The distal ring was centred on the leg and fastened to the Steinman pins. The wire was then tensioned. An oblique metaphyseal tibial osteotomy directed towards the superior tibio-fibular joint was made at the level of tibial tuberosity. Osteotomy initiated with fine k wire in the planned direction on medial aspect of tibia under C-ARM guidance and was completed with an osteotome. This was inserted through a 1-cm incision in the skin and blunt dissection was performed down to bone.The completion of osteotomy was ascertained radiographically and clinically. The proximal and distal ring was connected with one telescoping rod on medial aspect and 2 hinges on lateral aspect lying at the level of osteotomy. Incision sutured in layers. Pin track dressing and incision dressing done. All screws tightened Post-operative Protocol: Antibiotics and Intravenous fluids are given for the initial 2 post operative days. Adequate analgesia is given, Regular sterile pin track dressing is done. Initially physiotherapy in the form of quadriceps strengthening and hamstring strengthening exercises are taught. Later partial weight bearing walker mobilization for 1 week, followed by partial weight bearing. This is continued for a period of 1 month. ,After 1 month patient asked for follow up. Follow up of the patient: At the end of 6 weeks patient is posted for another operative procedure for removal of external ring fixator and application of proximal tibia plate to prevent the osteteotomy collapse under spinal anaesthesia.
Post-operative protocol: antibiotics and Intravenous fluids are given for the initial 2 post operative days. Adequate analgesia is given and regular sterile pin track dressing is done. Initially physiotherapy in the form of quadriceps strengthening and hamstring strengthening exercises are taught. Weight bearing is started on the 2 nd day and patient is discharged on the 3rd day. Patient is asked for follow up after 6 months for proximal tibia plate removal.
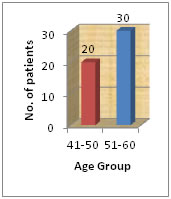
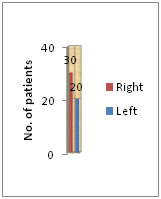
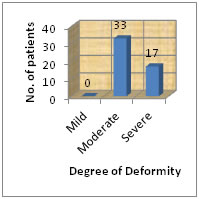
RESULTS Our study was conducted on 50 patients who came to us with the complaints of pain and deformity in their knee. On clinical and Radiographic examination they were diagnosed to have isolated medial compartment osteoarthritis of knee and operated with medial opening wedge high tibial osteotomy with an external ring fixator followed by application of proximal tibial plate. Out of 50 patients 22 were men and 28 were women. Side of Knee Involvement: The right knee is involved in 30 patients and left knee is involved in 20 patients. Degree of Deformity: The varus deformity in these patients were graded as mild (0-5 degree), moderate (5-10 degree) and severe (7-10 degree). Out of 50 patients 33 had moderate varus deformity and 17 had severe varus deformity. Radiographic measurements were made on each axis of the operated knee. The mechanical axis were calculated in each patient both pre and post operatively. The Mean mechanical axis in the pre and post operative group were statistically analysed with the help of student T test and the result were found to be statistically significant in these group (P=0.001) Pain was analysed using visual analogue scale both pre and post operatively on the visual analogue scale for pain, majority of the patient had score of 8 (40%), followed by 7 (30%) and 6 (20%) and 9 (10%). Post operatively majority of the patient had a score of 1 (25%) followed by a score of 2 (15%) and then score of 3 (10%). The pain score when compared on student T test was found to be decrease by 5 points after surgery.
Figure 1: C-arm image of olive wire insertion
Figure 2: (Proximal Tibia Plate Application at 6 Weeks) (Plate Removal After 6 Months) Figure 3: (knee ROM at day-2) (Partial Weight Bearing) (After Removal of Fixator)
Figure 4: Figure 5: Figure 6:
Table 1: Pre-operative Pain
Table 2: Post-operative Pain
Table 3: Comparison of Pre-operative and Post-operative Pain
Table 4:
DISCUSSION High tibial osteotomy is a time tested procedure in the treatment of medial compartment osteoarthritis of knee. Total knee replacement or unicompartmental knee replacement are not suitable in young healthy active patients with good functional activities. Our study mainly aimed to analyze the short term results of the surgery in our patients and its possible role in our social context. The main complaint for which our patients opted for surgery in our study is the untolerable pain and the disability causing restrictions in day to day activities. The goal of HTO is to reduce excessive loading of the medial compartment of the knee by correcting the varus deformity, thereby reducing pain and improving function. The biomechanical basis for the optimal degree of correction has been disputed and the recommended postsurgical knee alignment varies widely. There is a consensus among authors that slight overcorrection in HTO produces more satisfying results. However, the optimal degree of valgus angulation is still controversial. Valgus Angulation: Conventry MB et al12 reported that the 10-year survival rates were 63% in knees with 5º valgus angulation, 87% in knees with 6º-7º valgus angulation, and 94% in knees with ≥8º valgus angulation. In our study we gave a valgus angulationn of 3-5 degrees and after the one year follow up the pain in the knee joint was significantly reduced. In our study the mean pre-operative mechanical axis was around 168 degrees and mean post operative mechanical axis was around 180 degrees. This correction in the mechanical axis was beneficial in correcting the varus deformity in the patients with osteoarthritis of knee joint. Varus deformity of the knee causes pain in the patients and hence correction of the varus deformity will subsequently lead in the reduction of pain. Pain: In our study, the pain in the patient which was assessed by visual analogue scale decreased by an average of five points post operatively. This in turn led to the impro Hence, the precise estimation of the pre-operative deformity is mandatory since good results are closely correlated with accurate correction. In reporting long term results of high tibial osteotomy, Coventry12 evaluated 213 knees for deformity, pain, function and motion, more than 60% patients were relieved of pain and had good functions, even 10 yrs after the operation. The major complication reported was the recurrence of deformity which coincided with the recurrence of pain. Most authors have concluded that proximal tibial osteotomy’s reliability is approximately 6 years. Michelle Wolcott, Shaun Traub, and Chad Efird13 in their study on “High Tibial Osteotomy In The Young Active Patients” showed HTO as a treatment option for malalignment in the older, less active adult and has shown promising results in a younger, more active population. There was significant improvement in the pain following high tibial osteotomy in patients who had medial compartment osteoarthritis of knee joint. Medial wedge opening Osteotomy: We preferred medial opening osteotomy in our study because it implies multiple advantages over closing wedge osteotomy like, Fibular osteotomy not required. Limb is not shortened, patellofemoral junction is not altered. Knee Society Score: The knee society score in the post operative patients were found to be significantly improved when compared to the pre operative scores. Most of the patients in our study were having knee society score in the range of 80-100 which is considered to be excellent. The patients have significant improvement in the pain relief and can be able to sit cross leg and squat. Pfahler et al14 in their study on “long term results on high tibial osteotomy for medial osteoarthritis of knee” showed that 90% of the 49 patients had excellent knee society scores. External Ring Fixator: High tibial osteotomy with an external ring fixator in our study provided to be a good option as it avoids the complications associated with closed wedge osteotomy and also implant related complications when used in medial opening wedge osteotomy. The treatment with external fixator allowed us for accurate correction of the varus deformity leading to realignment of the mechanical axis such that the weight bearing line passes through the fujisawa point ie lateral tibial spinous process of the knee. The mean mechanical axis post operatively was 180 degree compared to the preoperative axis i.e. 169 degree and statistical analysis proved to be statistically significant (p=<0.001).
CONCLUSION High tibial medial opening wedge osteotomy is a good procedure for the treatment of medial compartment osteoarthritis of knee in the young and middle aged individuals. The further progression of osteoarthritis can be prevented and further knee replacement can be averted. Accurate and controlled correction of mechanical axis can be achieved with this surgery. High tibial osteotomy does not hinder future total knee arthroplasty procedure. Appropriate patient selection, good pre operative planning and precise surgical techniques are essential for success of HTO. Therefore medial opening wedge HTO with a external ring fixator followed by application of proximal tibia plate should be recommended for the treatment of degenerative arthritis of the knee in young and middle aged active patients for symptomatic improvement and maintenance of activity levels.
REFERENCES
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||


 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.