 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 8 Issue 2 - November 2018
Prevalence of vitamin D insufficiency in an adult normal population of India
C Ravi1*, Bachu Srinivas2, Kalwa Dinesh3
1Associate Professor, Department of Orthopedics, Mahavir Institute of Medical Sciences, Vikarabad, Telangana, INDIA. 2Associate Professor, Department of Orthopedics, Government Medical College, Nizamabad, Telangana, INDIA. 3Registrar, Apollo DRDO, Hyderabad, INDIA. Email: ravihyd9@yahoo.com
Abstract Background: There are multiple studies in different countries regarding the prevalence of vitamin d deficiency. These studies showed high prevalence of vitamin d deficiency in Asian countries. This study tries to elucidate the prevalence of vitamin d deficiency and its influencing factors in population of India. Objective: Vitamin d deficiency is recognized as a global public health problem, but the population‐based prevalence of deficiency and its determinants in Indian adults is less known. This study evaluated the vitamin d status of Indian adults aged ≥20 years and risk factors associated with vitamin d deficiency in this population. Methods: 1873 subjects above 20years old were randomly selected. 25 (oh) d serum levels were measured. patients were divided into two groups depending on the presenting symptoms. Measurements: Serum concentrations of 25‐hydroxyvitamin d [25(oh)d] were measured by immunoassay. Vitamin d deficiency was defined as a concentration <10 nmol/l. Information on demographic and lifestyle factors was derived from interview‐administered questionnaires. Result: A high percentage of vitamin d deficiency was defined in the study population. prevalence of severe, moderate and mild vitamin d deficiency was 9.5%, 57.6% and 14.2% respectively. In 1873 patients, 972(51.8%) are male and 901(48.1%) are female, out of 972 patients 284(29.2%) patients were found to have deficient vitamin D levels. Out of 901 patients 292(32.4%) patients were found to have deficient vitamin D levels. Out of 1873 patients tested, 605(32.3%) patients were found to have insufficiency of vitamin D levels, 576(30.8%) patients were found to have deficiency of vitamin D levels. Conclusions: Vitamin d deficiency has a high prevalence in India. It is important to pay attention to this rather high prevalence of vitamin d insufficiency in the general adult population. In order to avoid complications of vitamin d deficiency, supplemental dietary intake seems essential. This indicates that strategies are needed at the population level to improve vitamin d status of Indians.Key Words: Vitamin d vitamin d deficiency calcium intake sunlight exposure, normal population; parathyroidhormone.
INTRODUCTION Over a period of last decade and last four years in particular the awareness of Vitamin D deficiency has increased considerably, not only among the treating doctors but also in patient and general public. The deficiency of vit d is more than initial expectations. Mounting evidence suggests that vitamin D deficiency could be linked to several chronic diseases, including cardiovascular disease4 and cancer. The purpose of this study was to examine the prevalence of vitamin D deficiency and its correlates to test the hypothesis that vitamin D deficiency was common in the Indian population. Vitamin D is an essential element for establishing and maintaining bone structure. Vitamin D deficiency results in rickets and osteomalacia. Even slight vitamin D deficiency results in secondary hyperparathyroidism and increased bone resorption. In addition, there has been increased attention to the physiologic importance of vitamin D in non-skeletal tissues. Vitamin D is supplied by consumption of vitamin D-rich foods and by vitamin D synthesis in skin. Natural nutrient materials are not a sufficient source of vitamin D to supply the body requirements; therefore where there is no supplementation of foodstuffs, the main source for vitamin D is produced by UV light. Regarding the significant role of sunlight in vitamin D synthesis, it is quite logical to suggest low prevalence of vitamin D deficiency in tropical countries. However the studies carried out in the preceding two decades have shown a high prevalence of vitamin D deficiency in tropical countries such as China, Turkey, India, Iran and Saudi Arabia. The prevalence of vitamin D deficiency varied between 30% and 93%. However, the majority of these studies were limited to specific age and sex groups. Therefore, elucidation of vitamin D status at the community level and in different climates of a country seems essential. Survey 2017-18 data were analyzed for vitamin D levels in adult participants (N = 4495). Vitamin D deficiency was defined as a serum 25-hydroxyvitamin D concentrations ≤20 ng/mL (50 nmol/L). The overall prevalence rate of vitamin D deficiency was 41.6%, with the highest rate seen in blacks (82.1%), followed by Hispanics (69.2%). Vitamin D deficiency was significantly more common among those who had no college education, were obese, with a poor health status, hypertension, low high-density lipoprotein cholesterol level, or not consuming milk daily (all P<. 001). Multivariate analyses showed that being from a non-white race, not college educated, obese, having low high-density lipoprotein cholesterol, poor health, and no daily milk consumption were all significantly, independently associated with vitamin D deficiency (all P <. 05). The concept of vitamin D `insufficiency' which has a biological effect on calcium homeostasis and skeletal metabolism needs to be distinguished from the concepts of both vitamin D `deficiency' which leads to osteomalacia and vitamin D `sufficiency' which has no effect on calcium homeostasis. The threshold of the serum 25(OH)D concentration that separates vitamin D sufficiency for insufficiency can be designed from biological effects, in particular the increase in serum parathyroid hormone (PTH) secretion9 and the conversion of 1,25(OH)2D from 25(OH)D. The increased secretion of PTH in vitamin D insufficiency is well documented and contributes to bone fragility and probably to bone fractures in the elderly through increased bone turnover. In summary, vitamin D deficiency was common in the Indian population. Given that vitamin D deficiency is linked to some of the important risk factors of leading causes of death in the United States, it is important that health professionals are aware of this connection and offer dietary and other intervention strategies to correct vitamin D deficiency.
MATERIALS AND METHODS Study conducted in and around Vikarabad and Hyderabad, of Telangana state in India. Study was conducted from June 2016 to June 2018. The study was approved by institutional ethical committee. Informed consent was obtained from all the participants, after explaining about Vitamin D deficiency and purpose of study. The study consists of 2 groups of people Group 1: Bone pains Group 2: No specific complaints, suggests randomized control Inclusion Criteria: Patients with vague symptoms, bone pains, generalized malaise. Patients of both genders were included. Exclusion Criteria: Previous vit d therapy, hepatic or renal disease, metabolic bone disease, malabsorption, sterility, oligomenorrhea, type I diabetes, hypercortisolism, malignancy, immobility for more than four weeks, pregnancy, lactation, and medications influencing bone metabolism 1873 selected subjects participated in this study, Sampling was performed after taking informed consent, one fasting blood sample was taken from each participant. Then samples were sent to the laboratory for analysis. 25-hydroxy vitamin D (25(OH) D) level was measured with RIA method.
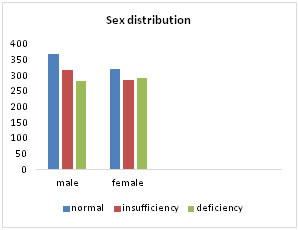
RESULTS To facilitate interpretation of the results from, these were grouped into following Table 1: Sex related distribution
Table 2: Age distribution
Table 3: General population distribution
Out of 1873 patients tested, 605(32.3%) patients were found to have insufficiency of vitamin.d levels, 576(30.8%) patients were found to have deficiency of vitamin.d levels. In 1873 patients, 972 are male and 901 are female, out of 972 patients 284 patients were found to have deficient vitamin.d levels. Out of 901 patients 292 patients were found to have deficient vitamin.d levels. Figure 1:
DISCUSSION In our study the prevalence of severe and moderate vitamin D deficiency was 32.3% had insufficiency and 30.8 had deficiency. With the increase in awareness and importance of Vitamin D deficiency, followed by treatment the profile of vit d deficiency started changing. Numerous epidemiologic studies suggest that exposure to sunlight, which enhances the production of vitamin D3 in the skin, is important in preventing many chronic diseases, unrecognized epidemic of vitamin D deficiency worldwide is a contributing factor of many chronic debilitating diseases. A cross-sectional study demonstrated associations between vitamin D deficiency and both higher disease activity and functional impairment in axial spondyloarthritis14 Vitamin D deficiency is associated with a reduction of lymphocyte subsets and altered T-lymphocyte activation which are considered to be risk factors for neonatal infection.15 Several studies have shown a high prevalence of vitamin D deficiency in individuals with CKD. Low vitamin D levels upregulate the renin-angiotensin-aldosterone system (RAAS), cause endothelial dysfunction, and increase inflammation.16 Vitamin D deficiency is universal among patients with chronic liver disease, and at least one-third of them suffer from severe vitamin D deficiency.17 Vitamin D deficiency occurs frequently in COPD and correlates with severity of COPD(chronic obstructive pulmonary disease)18 New evidence supports a potential role for vitamin D in maintaining innate immunity and preventing diseases such as diabetes and cancer.19 Annual measurement of serum 25(OH)D is a reasonable approach to monitoring for vitamin D deficiency. The recommended adequate intakes for vitamin D are inadequate, and, in the absence of exposure to sunlight, a minimum of 1000 IU vitamin D is required to maintain a healthy concentration of 25(OH) D in the blood. In countries where vitamin D fortified foodstuffs are available (USA and some Scandinavian countries), prevalence of vitamin D deficiency is less when compared to European countries10. In European countries where there is no vitamin D supplementation, deficiency is more prevalent. Vitamin D deficiency prevalence is much higher in Asian countries. Vitamin D has a long half-life and its frequent prescription especially in elderly women with musculo-skeletal complaints can explain differences in serum vitamin D. Regarding the essential role of sunlight in vitamin D synthesis, it is unexpected to see a high prevalence of vitamin D deficiency in countries such as Saudi Arabia. Recommended dietary allowance:12,13
Table 3:
I.U-international units.
Different hypotheses can be made such as insufficient sun exposure, clothing habits, hyper pigmentation, air pollution, insufficient intake of vitamin D and special dietary habits. Although sunlight plays an essential role in vitamin D synthesis, its' role in vitamin D deficiency of Asians is not obvious. In the present study sun exposure was not significantly different between subjects with vitamin D deficiency and those with normal vitamin D status probably reflecting the effect of level of pigmentation. Although there is sufficient sunlight in all seasons in India half of people who had more than 30 minutes of sun exposure had vitamin D less than 8 ng/ml (20 nmol/l). Holick1,2,3and colleagues showed similar rate of vitamin D synthesis in Asians as of Europeans; but Asians required greater duration of exposure, probably related to pigmentation. Other studies showed the same degree of increase in 25 (OH) Din summer months in Asians compared with Europeans. Insufficient vitamin D intake is another hypothesis for high prevalence of vitamin D deficiency in Asians. In the Omdahl7 study, daily vitamin D intake in elderly healthy women was 54 units. Decreased dietary calcium level induces increased serum PTH level and increased catabolism of 25 (OH) D, therefore decreased 25(OH) D is induced by dietary calcium deficiency. The urban society has low Calcium and vitamin D intake in view of the reduced consumption of dairy products and increase in intake of fast food along with sedentary life, smoking and alcohol abuse.11 Awumey8 et al showed higher activity level of 24-hydroxylase in fibroblasts of Indian-Americans compared with controls. Therefore, increased vitamin D catabolism may cause vitamin D deficiency in Asians. In order to elucidate specific etiologies responsible for high prevalence of vitamin D deficiency in Asians further studies should be carried out. It is possible that vitamin D deficiency is induced by combination of above mentioned etiologies. In order to clarify the significance of each etiologic factor, randomized controlled trials are necessary.
CONCLUSION It is found that overall vitamin-d deficiency and insufficiency is 60%. As against the conventional studies. It is found that patients with bone pains, joint pains responded to vitamin-d supplements by complete or near complete symptoms particularly in young patients. Other patients who had partial improvement had other comorbidities invariably further studies are required to ascertain the importance and contribution of vitamin-d. Given the high prevalence of vitamin D deficiency in India, effective solution to overcome its consequences seems indispensable.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.