 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 9 Issue 1 - January 2019
Functional outcome in distal radius articular fractures treated by external fixator with k-wires versus volar-locking plating- A comparative study
Rishabh Kumar1*, Satendra Kumar Sinha2, Anand Shankar3, Satyendra Kumar4
1Senior Resident, 2Professor & HOD, 4Post Graduate trainee, Department of Orthopaedics, Nalanda Medical College and Hospital, Patna, Bihar, INDIA. 3Consultant, Patna Bone and Spine Hospital, Patna, Bihar, INDIA. Email: drrishabh2005@gmail.com
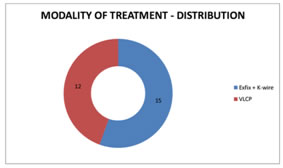
Abstract Purpose: The purpose of this study was to compare the functional out come in distal radius articular fractures treated by closed reduction through bridging external fixator augmented with k-wires and volar-locking plating. Methods: This study included patients with comminute dunstable intra-articular distal radius fractures treated at Nalanda Medical College Hospital. 27 patients treated with either modality of treatment were analysed, who had been followed up for an averageofwas8.9 months, (range :3monthsto18 months).Prospective and retrospective data were gathered on patients, of which 15 were treated with external fixator augmented with k-wire and12weretreatedwith2-columnfixed angle volar LCP. The 2 groups were compared for range of motion(ROM), strength, and functional out come as measured by the Mayowrist score. Fracture reduction was evaluated from radiographs taken at the last follow-up visit and compared between groups. Sarmiento’s modification of Lindstorm’s criteria was used to compare the radiological out come in both the groups. Results: The mean passive wrist ROM at the final follow-up evaluation in extfixation patients was 55 degrees extension and 67 degrees flexion, compared with 69 degreesextensionand77degreesflexioninpatientstreatedwithvolar LCP group. Whereas mean passive wrist ROM at the final follow-up evaluation in extfixation patients was 58 degrees supination and 46 degrees pronation, compared with 76 degrees supination and 64 degrees pronation in patient streated with volar LCP group. Final radiographic measurements for the Extfixation group averaged 2.9 degrees volartilt and14.2 mm degrees radial inclination, with 5 mmradial length. The Volar LCP group averaged 7.3 degrees volartilt, 16.9 degrees radial inclination, with 9.75 mm radial length. Radial length and volartilt were significantly greater for the ORIF group when compared with the radial length. There was significant difference in the radiological and functional outcome of AOM uller type C fractures treated by volar LCP with respect to the externalfixator group (p value 0.009 and 0.026 respectively). There was no significant difference in the radiological and function a outcome of AOM uller type B fracture streated byv olar LCP with respect to the external fixator group(pvalue0.706and0.707 respectively). Key Word: distalradius fractures, externalfixator, k- wires, volar LCP, functional assessment, May owrist score
INTRODUCTION Distal radius fractures are most common fractures of upper limb presenting at emergency rooms, compromising of more than 16% of all fractures. Distalradial fractures have abimodal type of age distribution with high-energy trauma contributing in younger and low energy traumain elderly population. Females are more liable to distal radius fractures when compared with males mainly because of more severe osteoporosis and a higher liability of elderly women to falls compared to the age-matched men. The metaphyseal widening of the distal radius is a zone predisposed to fracturesbecauseofaloweramountofstrongcorticalboneandhigheramount of weaker can cellous bone. The major risk factors are low bone mineral density (BMD) and at endency to fall. It was clinically proved that intra-articular step-off and radial shortening corrected by surgery had improved patient out come. These issues don’t affect elderly people and low-demand patients probably due to low functional and physical demand. In general anatomic reduction should be pursued in younger and high-demand elderly patients (because of longe healing time and to initiate early mobilization) with extra-articular fracture or intra-articular fractures. Low demand elders with severely displaced in prearticular fracture or median nerve compression requires urgical management but otherwise the prime focus in this group should be on joint movement. Non-displaced or reducible but stable extra and intra-articular fracture scan also betreated with casting. Unstable reducible extra-articular fractures are commonly treated with reduction and often supplemented with extra-or intra-focal pinning. Extra-articular fractur es that are irreducible, intra articular fractures and fractures for demanding patients who require early mobilization, are commonly treated with plating(more often with palmar plating),intra medullary fixation, external fixation or pinning. Close reduction and cast immobilization has been the principal mode of management of distalradius fractures but it often lead to fracture malunion and sub luxation/dislocation of distal radioulnar joint, hence resulting in poor functional, radiographic and cosmetic results. Open reduction and volar plating was designed to ensure more consistent correction of displacement and maintenance of reduction. Metaphy seal defect scan also be grafted, although not generally advocated in fresh fractures and good bone quality.
AIM The aim of this study was to compare the Functional outcome in distal radius articular fractures treated by external fixator with k-wires with those treated by volar-locking plating using the Mayo wrist score.
MATERIAL AND METHODS A comparative study of the functional outcome in distal radius articular fractures of 27 patients treatedbyclosedreductionthroughbridgingexternalfixatoraugmentedwith K-wires and volar-locking plating was done. The criteria for patient selection were, Inclusion Criteria
Exclusion Criteria
Patients of both sexes were recruited in the study according to the devised inclusion and exclusion criteria.
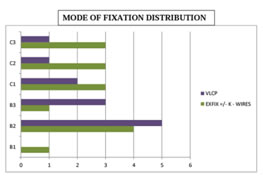
RESULTS The mean followup was 8.9 months, ranging from 3 months to 24 months. All 27 patient shadregular follow-up. UNION: All the patients had good union. The mean time of union was 14 weeks with arrange of 10 to 18 weeks with a 16 case shealing by12 weeks. Rest of the 11 cases took alonger duration. 1 case of delayed union was reported in the external fixator group when the external fixator was removed and a cast was applied for a further 2 months till union was complete. Longer duration to union is noted in patients of older age with relatively poor bone quality. MALUNION: 3 patients of the 15 treated with kirschner wire augmented External fixator had mal union with significant dorsalangulation with negative palmartilt. Table 1: Fracture Classfication
Figure 1: Figure 2:
Table 2: Subjective evaluation of patients by mayo score
Table 3:
In our study we had 27% of external fixator and 42% of Volar LCP associated with very good results based on Mayo wrist score. Table 4:
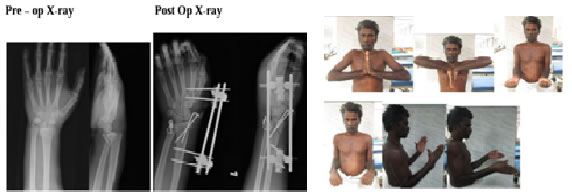
Case 1: Case 2:
CONCLUSION Functional results is different from Radiographic results. Both the External fixator and Kwires and locking plating methods have their individual place in the management of distal radius fractures and the needs of the patient, his age, functional requirement, expectations, side handedness all play a role in the decision making. Treatment should be on one to one basis and tailor made for the patients.
REFERENCES
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.