 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 9 Issue 3 - March 2019
Sujana Theja J S1*, Kiran Marathe2, B Gurumurthy3, Pavankumar Patted4
1,3Assistant Professor, 2Senior Resident, 4Junior Resident, Department of Orthopaedics, JSS Medical College, JSS Academy Of Higher Education and Research, Mysuru, Karnataka, INDIA. Email: drsujantheja@gmail.com
Abstract Background: Intertrochanteric hip fractures account for approximately half of the hip fractures in the elderly and pose a number of management dilemmas depending on the fracture configuration and status of the bones. A wide variety of implants are available for the internal fixation of these fractures ranging from dynamic hip screw which can be combined with trochanteric stabilisation plate; locking plates; intramedullary implants such as proximal femoral nail (PFN), trochanteric femoral nail (TFN) and Gamma nail. A study was undertaken to evaluate the surgical management of intertrochanteric fractures with intramedullary trochanteric femoral nail (TFN) design and dynamic hip screw (DHS) as fixation devices and to determine the rate of union, complications, operative risks and functional outcome and co morbidities associated with intertrochanteric fractures. Materials and methods: The fractures were classified according to Boyd and Griffin classification system. 60 cases of intertrochanteric fracture were managed surgically using Trochanteric femoral nail (n=30) and dynamic hip screw (n=30). The results were analyzed according to age, type of fracture, operative details and final outcome using Kyles criteria. Results: In our study, 30 cases treated with Trochanteric femoral nail had better results than 30 cases treated by Dynamic hip screw, in terms of operating time, surgical exposure, blood loss, range of movements and complication rates. At the final follow-up of 6 months, excellent outcome was seen in 73.3% of patients treated with Trochanteric femoral nail as compared to 56.7% of patients treated with Dynamic hip screw. Conclusion: Trochanteric Femoral nail is a superior implant for stable and unstable intertrochanteric fractures in terms of operating time, surgical exposure, blood loss, and complication rates. Key Word: Intertrochanteric fractures; BOYD and GRIFFIN’s classification; Trochanteric femoral nail; Dynamic hip screw, Femur fracture.
INTRODUCTION Hip fractures are very common among the elderly population, mainly because of increasing incidence of osteoporosis, especially in developing countries like India. Of all hip fractures, proximal femoral fractures seem to be most common and intertrochanteric fractures being major part of it. The goal of treatment of any intertrochanteric fracture is to restore mobility safely and efficiently while minimizing the risk of medical complications and technical failure and to restore the patient to preoperative status. There are multiple factors and variables, which affect the biomechanical strength of repair. Patient dependent variables are bone quality, which is related to age and osteoporosis, and fracture pattern and fracture stability. Surgeon dependent variables are quality of fracture reduction and choice and placement of implant. Unstable intertrochanteric fractures are technically much more challenging than stable fractures; a stable reduction requires providing medial and posterior cortical contact between the major proximal and distal fragments to resist varus and posterior displacing forces. In the treatment of stable intertrochanteric fracture patterns, lag screw and side plate constructs have become the implant of choice.1 Many studies have reported predictable stability and healing in these stable fracture patterns.2 However, unstable fracture patterns with posteromedial instability remain a persistent challenge3. Mechanical failure including loss of purchase of the compression screw within the femoral head, pulling off of the side plate, and disengagement of the screw and barrel has been reported to occur in as many as 28% of fractures3,4 Additionally, over-impaction of the fracture fragments with lag screw and side plates may lead to significant loss of limb length and delays in rehabilitation and ambulation.5 Cephalomedullary devices for the treatment of unstable intertrochanteric fractures have several theoretical advantages over side plate implants. Biomechanically, a shorter lever arm between the rotational centre of gravity of the hip and the femoral fixation component leads to a stronger construct. It is a more biological device. Cephalomedullary fixation may help prevent excessive shortening from collapse, in that the nail acts as a calcar and lateral wall replacement to support the femoral neck. Insertion of the nail through the tip of the greater trochanter requires less dissection and may lead to less blood loss and fewer wound complications, as well as earlier postoperative recovery6 Dynamic Hip Screw (DHS) has been well established and studied as implant of choice for Trochanteric fractures from many years. There are few literature reviews studying the efficacy of the newly introduced intramedullary device- Trochanteric Femoral Nail (TFN) which is a better biomechanical weight shearing design especially for unstable intertrochanteric fractures. There are hardly any study comparing these extra medullary (DHS) and intramedullary (TFN) implants for fixation of intertrochanteric fractures of different patterns and thus the present study.
MATERIALS AND METHODS After approval of institute ethical committee and obtaining consent, 60 Patients coming to the emergency department or outpatient of orthopaedic department, with Intertrochanteric fractures of Femur, JSS Hospital, Mysore between September 2012 to June 2018, were enrolled for study. The following patients were included, all patients above 50 years presenting with Intertrochanteric Fractures of Femur who were surgically fit.
The following patients were excluded from study
All the patients were carefully evaluated preoperatively which included detailed history to determine the cause of fracture and other diseases. The radiograph of pelvis with both hips and lateral view of the affected hip was taken. The fracture was classified using Boyd and Grifin classification. Skin traction was applied to all cases. The implant was selected based on computer generated random numbers. For TFN Nail diameter was determined by measuring diameter of the femur at the level of isthmus on an X-ray AP view, Neck shaft angle was measured in unaffected side in X-ray AP using goniometer and a standard length TFN (180 mm) was used in all our cases. For DHS Length of compression screw is measured from tip of the head to the base of greater tronchanter on X-ray AP view subtracting magnification, neckshaft angle Neck shaft angle is determined using goniometer on X-ray AP view on unaffected side and length of side plate is determined to allow purchase of atleast 8 cortices to the shaft distal to the fracture. post operative protocol: Isometric quadriceps exercise was started on day 2.Early hip and knee ROM were started as tolerated by the patient. Patients with TFN were mobilized and made to walk 20% weight bearing (toe touch) using a walker at the end of first week as tolerated by patient. Patients with DHS were mobilized when patient were pain free and made to walk 20% weight bearing (toe touch) using a walker by end of first week. Full weight bearing without support was allowed after radiological and clinical signs of union. Follow up was done 1st, 2nd, 3rd, and 6 months. The important parameters assessed were: 1.Clinical: Wound condition, Kyles scoring, Shortening. 2.Radiological: Union , Amount of collapse, Complications like screw cut out and Z- phenomena
OBSERVATIONS AND RESULTS The study involved 60 cases of intertrochanteric femur of either sex from September 2012 to June 2018. Out of 60 cases, 30 were treated by a dynamic hip screw and 30 were treated by trochanteric femoral nail. In our study, the mean age of the patient in the study was 68.52 ± 6.831, minimum being 53 years and maximum being 82 years. . There were 32 male and 28 female patients. The fracture due to domestic fall occurred in 36 patients (60%), 5 patients (8.3%) met road traffic accident, 19 patients (31.7%) had fall at work place. The right side was involved in 31 cases while left side in 29 cases. The Singh’s index for osteoporosis showed that there were 10 patients with grade 4 and above.
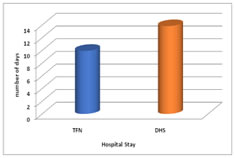
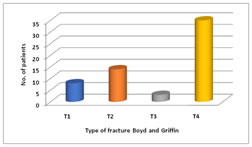 All the fractures were classified as per the Boyd and Griffin classification. There were 8 (13.3%) patients of type 1, 14(23.3%) patients of type 2, 3(5%) patients of type 3, 35(60%) patients of type 4 fractures. The mean duration of the surgery for TFN was 46.50 min and DHS was105.33 min which showed significant difference in the duration of both the implants. The mean duration of hospital stay for TFN was 9.93 days where as for DHS it was 13.33 days which statistically showed significant difference.
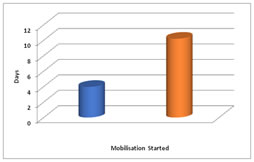
 In our study, patients operated with TFN tolerated mobilisation as early 3rd day (mean3.9667days) which significant when compared to the other group(mean 10.2 days). In our study, we could start full weight bearing in patients with TFN early (mean=2.4 weeks), than in patients with DHS (mean=7.9 weeks).
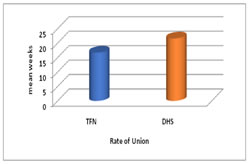
4 patients operated with TFN developed superficial infection only while 6 patients of DHS developed superficial infection and 4 patients developed deep infection. Pain VAS score assessed at 6 months showed 22 patients of TFN and 18 patients of DHS had Score 0f 0, 8 patients of TFN and 11 patients of DHS had score of 2, no patient of TFN and 1 patient of DHS had score of 4, which showed significant difference between the two groups. Limb Length Discrepancy (in cm) at 6 months was assessed which showed that 22 patients of TFN and 10 patients of DHS had no limb length discrepancy, 8 patients of TFN and 12 patients of DHS had limb length discrepancy of 1 cm, 8 patients of DHS had limb length discrepancy of 2 cm. 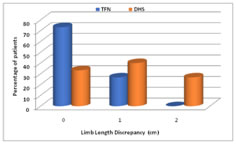 ROM at 6 months showed full range of movements in all patients of TFN group and 22 patients of DHS group, 7 patients of DHS group had 25% restriction and 1 patient had 50% restriction. The mean duration of rate of union in TFN is 16.7 weeks while in DHS it was 21.6 week.
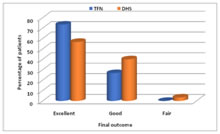
 The functional outcome was assessed based on KYLE’s criteria, 22 patients of TFN and 17 patients of DHS had excellent outcome, 8 patients of TFN and 12 patients of DHS group had good outcome,1 patient of DHS group had fair outcome.
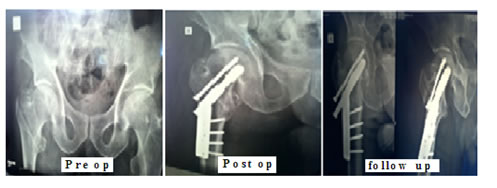
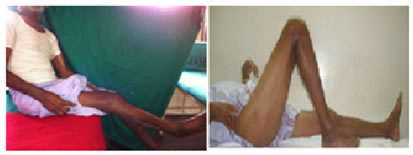
 Case 1 (TFN)  Follow up at 6 months  Case 2 (DHS)  Follow up at 6 months  Case 3 (TFN)  Follow up at 6 months  Case 4 (DHS) Follow up at 6 months DISCUSSION Intertrochanteric hip fractures account for approximately half of all hip fractures in the elderly population. Among these fractures, 50–60% are classified as unstable. Several methods of fixation have been proposed for the management of intertrochanteric fractures. The main objective of this study was to assess whether there are differences in functional recovery of elderly patients, rate of union, implant failure, post-operative complications after treatment of intertrochanteric fractures with two distinct, well-established fixation techniques. The intramedullary TFN tolerates greater static loads and much greater cyclic loading than the DHS device. Consequently, the fracture consolidates with TFN treatment even in the absence of primary restoration of medial support, as the implant temporarily compensates the function of the medial column. TFN reduced the distance between the hip joint and the implant, which diminishes the bending moment across the implant-fracture construct. Thus, more stability is provided. Early mobilization after surgery could reduce complications such as pneumonia, thromboembolic complications and pressure sores, as well as length of hospital stay in TFN than DHS. We found trochanteric femoral nail to be more useful in unstable patterns due to the fact that it has better axial telescoping and rotational stability as it is a load sharing device. Kyle et al7 in his extensive study of the biomechanical principles of the sliding hip screw has identified key factors that promote sliding. A reduction in the bending forces is vital since bending forces reduce slide and cause jamming of the implant. The bending forces are increased by Longer extension of the screw, Smaller screw angles and Heavier patients. In his subsequent studies on the sliding in second generation locked nails, Kyle et al7has noted that increased forces are required to initiate sliding in intra medullary devices as compared to sliding hip screw with plate. Amongst all intra medullary devices the Gamma nail requires the largest force. The explanation lies in the barrel of the side plate, the barrel provides a free passage for the screw to slide, thus the longer the barrel length the less the forces required to initiate sliding. The average age incidence in our study was 68.8 years, which was comparable to study by Wasudeo M et al8 of 67 years. There was male sex preponderance seen in our study. Our study results are comparable to other Indian studies 9. Trochanteric fracture were more common in persons aged above 60 years, mechanism usually resulting from trivial fall either at home or at work place. In our study trivial fall was around 60%, comparable to other Indian studies. In the present study of 60 cases, right hip fractures were seen in 31 cases and left hip fractures seen in 29 cases. In studies conducted by R C Gupta10 right sided fractures were more common, where as in studies made by Kenzora et al11 and Cleveland et al12 left sided fractures were more common. In our study based on the Boyd and Griffin classification, 58.3% of fractures were type 4 Boyd and Griffin, being most common, 23.3% of fractures were type 2 Boyd and Griffin, 13.3% of fractures were type 1 Boyd and Griffin and 5% fractures were type 3Boyd and Griffin. Majority of patients (43.3%) were found to have Singh’s Index 3, which was comparable to study by Wasudeo et al8. Mean operating time in our study for TFN was 46.50 mins (SD=8.62) and mean operating time for DHS was 105.33mins (SD=12.02). The operating time for TFN is comparable to Wasudeo et al8, who had mean operating time of around 50 mins, which was significantly lower than for DHS. In our study the average duration of stay for patients treated with TFN was 9.93 days (SD=1.33), which is comparable to Wasudeo et al8 of 12(SD=3.1). The average duration of stay for patients treated with DHS was 13.33 days (SD=2.89), which is comparable to Richard Kyle7of 18 days. The finding that functional recovery in the first 6 months after surgery is significantly poorer after DHS treatment is important, because it is widely known that elderly patients require faster recovery. Saudan et al13 assessed social functioning and mobility scores at 3, 6, and 12 months after surgery with TFN or DHS. Although findings at intermediate months were not explained in the study text, at 1-year follow-up, the authors found no significant differences in terms of return to pre-fracture levels of ambulation and independence between the PFN-treated and DHS-treated groups. Thus, they concluded that intramedullary nails (such as the PFN) offer no advantage over extramedullary devices (such as the DHS) for the treatment of intertrochanteric fractures caused by low-energy trauma. In our study, 73.3% in TFN group had excellent outcome, 26.7% had good outcome, according to KYLE’s criteria, which is comparable to Wasudeo et al8.
CONCLUSION Successful treatment of intertrochanteric fractures depends on bone quality, patient age, general health, interval from fracture to treatment, treatment adequacy, comorbidities, fracture reduction and fixation stability. The dynamic hip screw (DHS) provides controlled compression at the fracture site. Excessive medialisation in the osteoporotic bone causes pain and deformity. The trochanteric femoral nail (TFN) acts as a buttress to prevent medialisation of the shaft and provides more efficient load transfer than does a sliding hip screw. TFN reduces stress concentration at the end of the nail. TFN is a superior implant for stable and unstable intertrochanteric fractures in terms of operating time, surgical exposure, blood loss and complication rates.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.